

Bone mineral density enhances use of clinical risk factors in predicting ten-year risk of osteoporotic fractures in Chinese men: the Hong Kong Osteoporosis Study
- PMID: 21234548
- PMCID: PMC3186888
- DOI: 10.1007/s00198-010-1490-0
Bone mineral density enhances use of clinical risk factors in predicting ten-year risk of osteoporotic fractures in Chinese men: the Hong Kong Osteoporosis Study
Abstract
This prospective study aimed to determine the risk factors and the 10-year probability of osteoporotic fracture in Southern Chinese men. The findings show substantial population differences in fracture incidence and risk prediction compared to the FRAX(TM) model, and the addition of BMD information to clinical risk factor assessment improved fracture risk prediction in Chinese men.
Introduction: Clinical risk factors with or without bone mineral density (BMD) measurements are increasingly recognized as reliable predictors of fracture risk. Prospective data on fracture incidence in Asian men remain sparse. This prospective study aimed to determine the risk factors and the 10-year absolute fracture risk in Southern Chinese men.
Methods: This is a part of the Hong Kong Osteoporosis Study. One thousand eight hundred ten (1,810) community-dwelling, treatment-naive men aged 50 years or above were evaluated. Baseline demographic characteristics, clinical risk factors and BMD were recorded. Ten-year risk of osteoporotic fracture was calculated using Cox proportional hazards models.
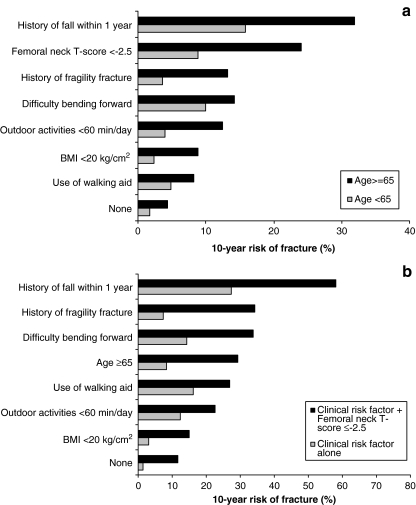
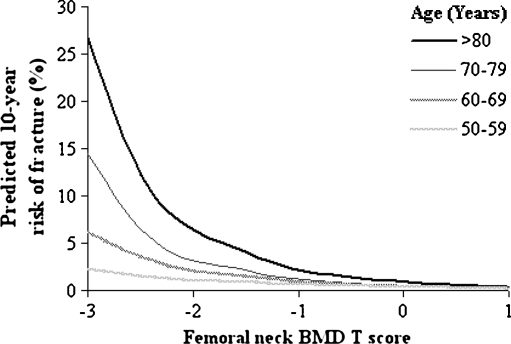
Results: The mean age of subjects was 68.0 ± 10.3 years. After a mean follow-up period of 3.5±2.9 years (range 1 to 14 years), 37 incident low-trauma fractures were recorded. The incidence for all osteoporotic fractures and hip fractures was 635/100,000 and 123/100,000 person-years, respectively. The most significant predictors of osteoporotic fracture were history of fall (RR 14.5), femoral neck BMD T-score < -2.5 (RR 13.8) and history of fracture (RR 4.4). Each SD reduction in BMD was associated with a 1.8 to 2.6-fold increase in fracture risk. Subjects with seven clinical risk factors and BMD T-score of -1 had an absolute 10-year risk of osteoporotic fracture of 8.9%, but this increased to 22.7% if they also had a femoral neck BMD T-score of -2.5.
Conclusions: These findings show substantial population differences in fracture incidence and risk prediction. The addition of BMD information to clinical risk factor assessment improved fracture risk prediction in Chinese men.
Figures



Similar articles
-
Ten-year fracture probability in Hong Kong Southern Chinese according to age and BMD femoral neck T-scores.Osteoporos Int. 2009 Nov;20(11):1939-45. doi: 10.1007/s00198-009-0906-1. Epub 2009 Mar 27. Osteoporos Int. 2009. PMID: 19326036
-
The added value of trabecular bone score to FRAX® to predict major osteoporotic fractures for clinical use in Chinese older people: the Mr. OS and Ms. OS cohort study in Hong Kong.Osteoporos Int. 2017 Jan;28(1):111-117. doi: 10.1007/s00198-016-3741-1. Epub 2016 Aug 26. Osteoporos Int. 2017. PMID: 27565645
-
Fracture risk prediction using FRAX®: a 10-year follow-up survey of the Japanese Population-Based Osteoporosis (JPOS) Cohort Study.Osteoporos Int. 2011 Dec;22(12):3037-45. doi: 10.1007/s00198-011-1537-x. Epub 2011 Jan 29. Osteoporos Int. 2011. PMID: 21279504
-
Prevalence and seasonal variation of hypovitaminosis D and its relationship to bone metabolism in healthy Hungarian men over 50 years of age: the HunMen Study.Osteoporos Int. 2013 Jan;24(1):179-86. doi: 10.1007/s00198-012-1920-2. Epub 2012 Mar 16. Osteoporos Int. 2013. PMID: 22422303 Review.
-
Nonalcoholic Fatty Liver Disease Is Associated With Decreased Bone Mineral Density in Adults: A Systematic Review and Meta-Analysis.J Bone Miner Res. 2023 Aug;38(8):1092-1103. doi: 10.1002/jbmr.4862. Epub 2023 Jun 12. J Bone Miner Res. 2023. PMID: 37254266
Cited by
-
Functional Restriction for the Fear of Falling In Family Caregivers.Medicine (Baltimore). 2015 Jul;94(27):e1090. doi: 10.1097/MD.0000000000001090. Medicine (Baltimore). 2015. PMID: 26166092 Free PMC article.
-
Osteoporosis knowledge, health beliefs, and self-efficacy in Hong Kong Chinese men.Arch Osteoporos. 2022 Apr 8;17(1):60. doi: 10.1007/s11657-022-01104-x. Arch Osteoporos. 2022. PMID: 35396655
-
Bone Mineral Density Screening Interval and Transition to Osteoporosis in Asian Women.Endocrinol Metab (Seoul). 2022 Jun;37(3):506-512. doi: 10.3803/EnM.2022.1429. Epub 2022 Jun 9. Endocrinol Metab (Seoul). 2022. PMID: 35678100 Free PMC article.
-
Vertebral fracture in postmenopausal Chinese women: a population-based study.Osteoporos Int. 2017 Sep;28(9):2583-2590. doi: 10.1007/s00198-017-4085-1. Epub 2017 May 30. Osteoporos Int. 2017. PMID: 28560474
-
Ethnic difference of clinical vertebral fracture risk.Osteoporos Int. 2012 Mar;23(3):879-85. doi: 10.1007/s00198-011-1627-9. Epub 2011 Apr 2. Osteoporos Int. 2012. PMID: 21461720 Free PMC article.
References
-
- Kanis JA, on behalf of the World Health Organization Scientific Group . Assessment of osteoporosis at the primary healthcare level. Technical report. UK: WHO Collaborating Centre, University of Sheffield; 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
