

Activated factor XI and tissue factor in chronic obstructive pulmonary disease: links with inflammation and thrombin generation
- PMID: 21236471
- PMCID: PMC3042502
- DOI: 10.1016/j.thromres.2010.11.005
Activated factor XI and tissue factor in chronic obstructive pulmonary disease: links with inflammation and thrombin generation
Abstract
Introduction: Increased cardiovascular mortality and risk of venous thromboembolism are serious extra-pulmonary complications of chronic obstructive pulmonary disease (COPD). Previously, circulating active tissue factor (TF) and factor XIa (FXIa) have been reported to be associated with acute coronary syndromes.
Objective: To measure plasma FXIa and active TF, prothrombin fragment 1.2 (F1.2), and markers of systemic inflammation (C-reactive protein [CRP], interleukin-6 [IL-6], tumor necrosis factor α [TNFα] and matrix metalloproteinase 9 [MMP-9]) in 60 patients with documented stable COPD free of previous thromboembolic events.
Methods: In-house clotting assays using inhibitory monoclonal antibodies against FXIa and TF.
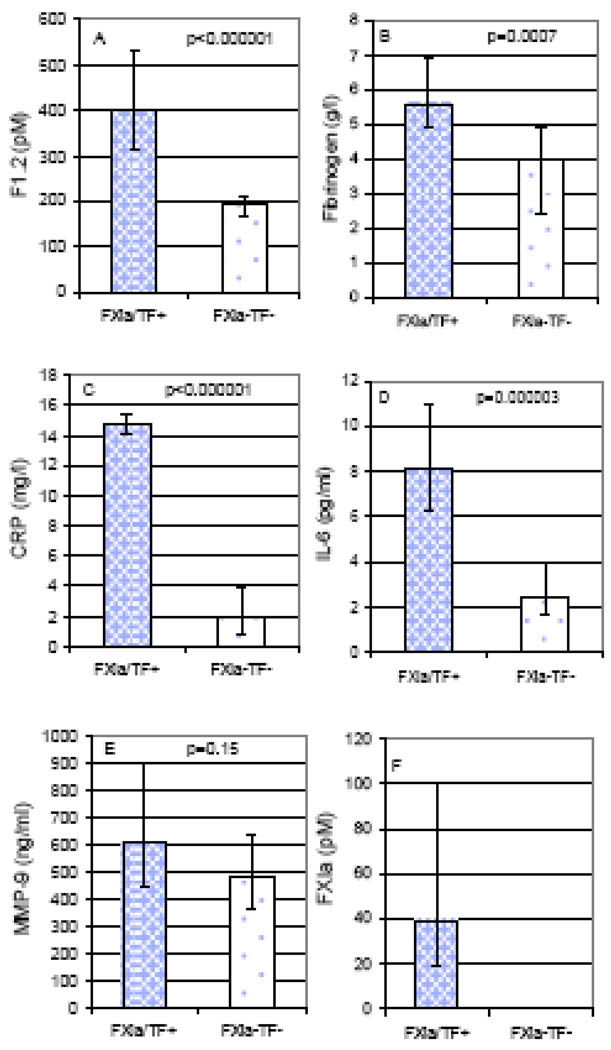
Results: FXIa was detected in 9 (15%) and TF activity in 7 (11.7%) COPD patients. Subjects positive for FXIa and/or TF (n=10; 16.7%) had higher F1.2 (median [interquartile range], 398 [216] vs 192 [42] pM, p<0.000001), fibrinogen (5.58 [2.01] vs 3.97 [2.47] g/L, p=0.0007), CRP (14.75 [1.20] vs 1.88 [2.95] mg/L, p<0.000001), IL-6 (8.14 [4.74] vs 2.45 [2.24] pg/mL, p=0.00002), and right ventricular systolic pressure (47 [15] vs 38 [12] mmHg, p=0.023), and lower vital capacity (66 [15] vs 80 [17] % predicted, p=0.04) than COPD patients without detectable FXIa and TF. COPD severity was not associated with the presence of circulating FXIa and active TF.
Conclusions: This is the first study to show that active FXIa and TF are present in stable COPD patients, who exhibit enhanced systemic inflammation and thrombin generation. Our findings suggest a new prothrombotic mechanism which might contribute to elevated risk of thromboembolic complications in COPD.
Copyright © 2010 Elsevier B.V. All rights reserved.
Conflict of interest statement
None declared.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease: Global strategy for diagnosis, management, and prevention of chronic obstructive pulmonary disease (updated 2009) www.goldcopd.com.
-
- Sin DD, Anthonisen NR, Soriano JB, Augusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28:1245–1257. - PubMed
-
- Sin DD, Man SF. Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation. 2003;107:1514–1519. - PubMed
-
- Butenas S, Orfeo T, Mann KG. Tissue factor activity and function in blood coagulation. Thromb Res. 2008;122 Suppl. 1:S42–S46. - PubMed
-
- Diamont M, Nieuwland R, Pablo RF, Sturk A, Smit JW, Radder JK. Elevated numbers of tissue factor exposing microparticles correlate with components of the metabolic syndrome in uncomplicated type 2 diabetes mellitus. Circulation. 2002;106:2442–2447. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
