

A randomized, placebo-controlled trial of abacavir intensification in HIV-1-infected adults with virologic suppression on a protease inhibitor-containing regimen
- PMID: 21239359
- PMCID: PMC3108099
- DOI: 10.1310/hct1106-312
A randomized, placebo-controlled trial of abacavir intensification in HIV-1-infected adults with virologic suppression on a protease inhibitor-containing regimen
Abstract
Background and objective: Maximizing the durability of viral suppression is a key goal of antiretroviral therapy. The objective of AIDS Clinical Trials Group Study 372A was to determine whether the intensification strategy of adding abacavir to an effective indinavir-dual nucleoside regimen would delay the time to virologic failure.
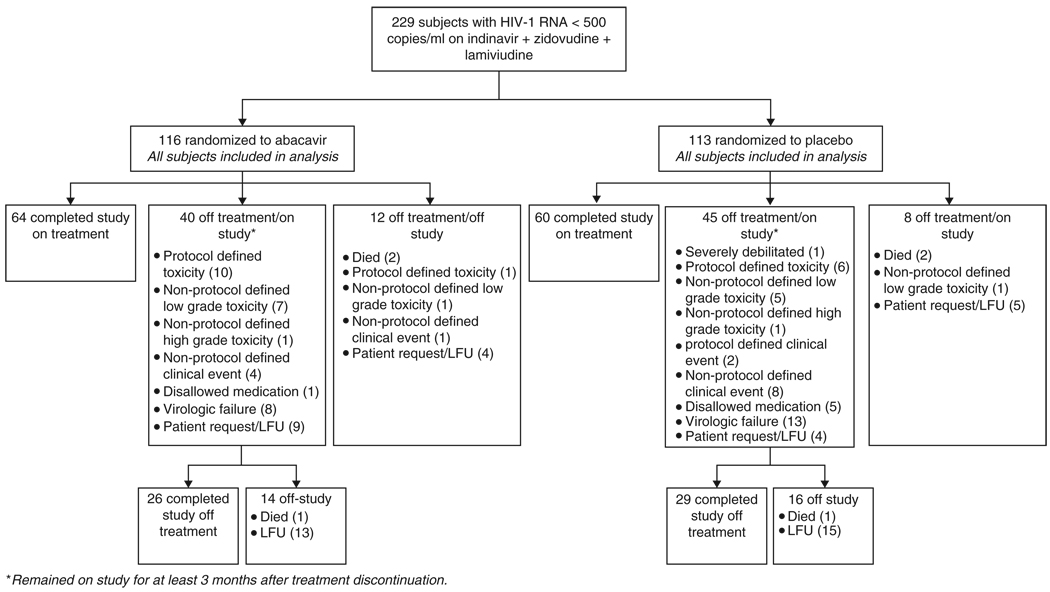
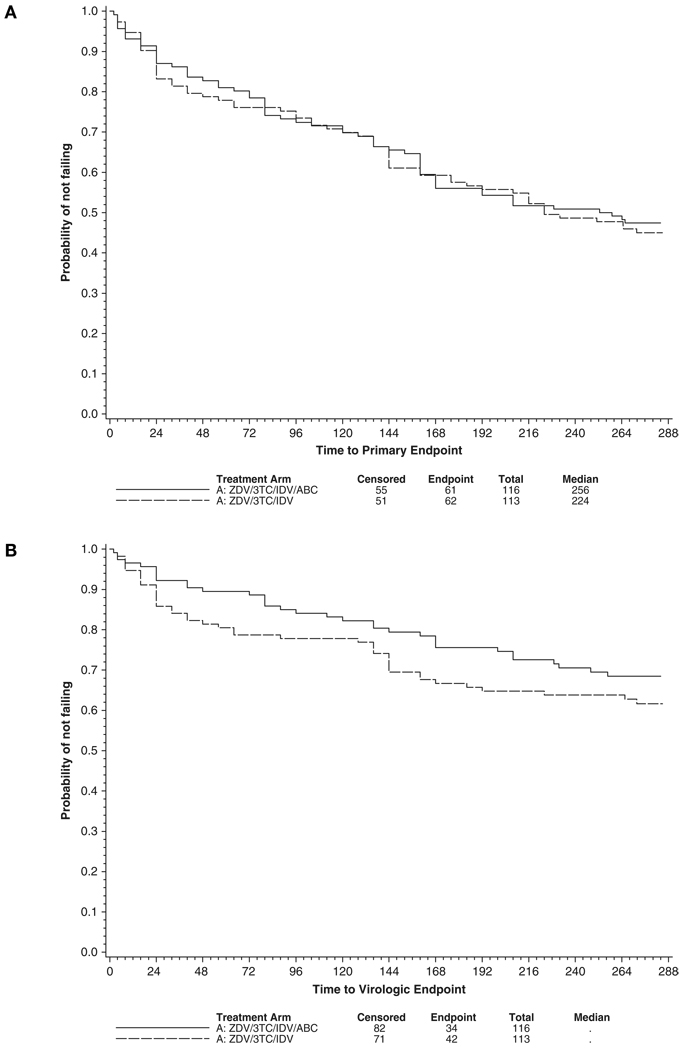
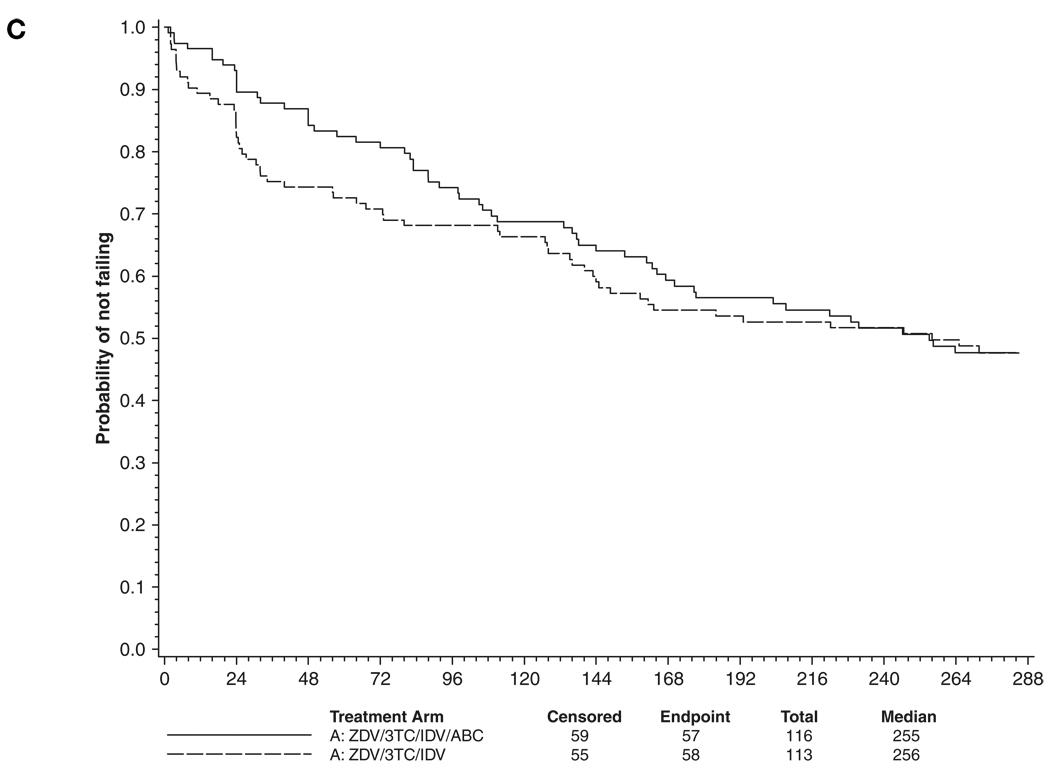
Methods: Zidovudine-experienced subjects (n=229) on therapy with indinavir + zidovudine + lamivudine with plasma HIV-1 RNA levels<500 copies/mL were randomized to abacavir 300 mg twice daily or placebo. The primary endpoint was the time to treatment failure, defined as a composite of confirmed virologic failure (2 consecutive HIV-1 RNAs>200 copies/mL) and treatment discontinuation.
Results: At baseline, the study population was 88% male with a median age of 41 years and median CD4 cell count of 250/mm3. Median follow-up was 4.4 years. The primary endpoint was reached in 61/116 of abacavir versus 62/113 of placebo recipients (P=.77); virologic failure occurred in 34/116 and 42/113 patients, respectively (P=.22). There were no differences in the proportions of subjects with plasma HIV-1 RNA levels below 50 copies/mL, in CD4 cell count increases, nor adverse events between the arms. In the study, 17% of subjects developed nephrolithiasis, 2% experienced abacavir hypersensitivity, and 4.8% experienced at least 1 serious cardiovascular event (7 [6%] in the abacavir arm, 4 [3.5%] in the placebo arm). In additional secondary and post hoc analyses, rates of intermittent viremia, suppression below a plasma HIV-1 RNA level of 6 copies/mL, and HIV-1 proviral DNA levels in peripheral blood mononuclear cells were not significantly different in the 2 arms.
Conclusions: The strategy of intensification with abacavir in patients who are virologically suppressed on a stable antiretroviral regimen does not confer a clinical or virologic benefit. As antiretroviral regimens have become more potent since this trial was completed, it will be even more difficult to prove that late intensification of already virologically suppressed patients will add benefit. However, studies are warranted with drugs with new mechanisms of action to determine whether the level of persistent viremia below 50 copies/ mL can be further reduced and what influence this may have on latent HIV reservoirs.
Trial registration: ClinicalTrials.gov NCT00000885.
Figures
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. [Accessed July 23, 2010];Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents. 2009 December 1;:1–161. http://www.AIDSinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.
-
- Thompson MA, Aberg JA, Cahn P, et al. Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA. 2010;304:321–333. - PubMed
-
- Demeter LM, Hughes MD, Coombs RW, et al. Predictors of virologic and clinical outcomes in HIV-1-infected patients receiving concurrent treatment with indinavir, zidovudine and lamivudine. AIDS Clinical Trials Group Protocol 320. Ann Intern Med. 2001;135(11):954–964. - PubMed
-
- Fang CT, Chang YY, Hsu HM, et al. Life expectancy of patients with newly-diagnosed HIV infection in the era of highly active antiretroviral therapy. Q J Med. 2007;100(2):97–105. - PubMed
-
- Degen O, van Lunzen J, Stellbrink HJ. Intensification of background antiretroviral therapy with abacavir during low-level failure may restore optimal suppression. Antivir Ther. 2000;5(2):91–94. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069424/AI/NIAID NIH HHS/United States
- P30 AI054907/AI/NIAID NIH HHS/United States
- U01 AI069477/AI/NIAID NIH HHS/United States
- RR023561/RR/NCRR NIH HHS/United States
- U01 AI069513/AI/NIAID NIH HHS/United States
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069423/AI/NIAID NIH HHS/United States
- AI069415/AI/NIAID NIH HHS/United States
- U01 AI069474/AI/NIAID NIH HHS/United States
- AI069465/AI/NIAID NIH HHS/United States
- AI069556/AI/NIAID NIH HHS/United States
- UM1 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069472/AI/NIAID NIH HHS/United States
- U01 AI069467/AI/NIAID NIH HHS/United States
- P30 AI050409/AI/NIAID NIH HHS/United States
- U01 AI069423/AI/NIAID NIH HHS/United States
- UM1 AI069513/AI/NIAID NIH HHS/United States
- RR 024160/RR/NCRR NIH HHS/United States
- M01 RR000046/RR/NCRR NIH HHS/United States
- AI069419/AI/NIAID NIH HHS/United States
- AI069511/AI/NIAID NIH HHS/United States
- AI032782/AI/NIAID NIH HHS/United States
- U01 AI027661/AI/NIAID NIH HHS/United States
- U01 AI069465/AI/NIAID NIH HHS/United States
- UL1 RR024996/RR/NCRR NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- AI069501/AI/NIAID NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- AI069532/AI/NIAID NIH HHS/United States
- AI069474/AI/NIAID NIH HHS/United States
- U01 AI069470/AI/NIAID NIH HHS/United States
- UM1 AI069495/AI/NIAID NIH HHS/United States
- U01 AI069484/AI/NIAID NIH HHS/United States
- UM1 AI069471/AI/NIAID NIH HHS/United States
- U01 AI069439/AI/NIAID NIH HHS/United States
- U01 AI069556/AI/NIAID NIH HHS/United States
- AI046370/AI/NIAID NIH HHS/United States
- UM1 AI069428/AI/NIAID NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- U01 AI069418/AI/NIAID NIH HHS/United States
- AI069423/AI/NIAID NIH HHS/United States
- AI54907/AI/NIAID NIH HHS/United States
- RR05096/RR/NCRR NIH HHS/United States
- U01 AI069428/AI/NIAID NIH HHS/United States
- U01 AI069532/AI/NIAID NIH HHS/United States
- UM1 AI069439/AI/NIAID NIH HHS/United States
- UM1 AI069415/AI/NIAID NIH HHS/United States
- M01 RR005096/RR/NCRR NIH HHS/United States
- AI069439/AI/NIAID NIH HHS/United States
- AI058740/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- UM1 AI069484/AI/NIAID NIH HHS/United States
- AI069428/AI/NIAID NIH HHS/United States
- UM1 AI069470/AI/NIAID NIH HHS/United States
- AI027665/AI/NIAID NIH HHS/United States
- U01 AI069501/AI/NIAID NIH HHS/United States
- AI2766/AI/NIAID NIH HHS/United States
- AI069452/AI/NIAID NIH HHS/United States
- R01 AI058740/AI/NIAID NIH HHS/United States
- AI069495/AI/NIAID NIH HHS/United States
- UM1 AI069477/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- AI069484/AI/NIAID NIH HHS/United States
- AI068636/AI/NIAID NIH HHS/United States
- U01 AI069450/AI/NIAID NIH HHS/United States
- AI073961/AI/NIAID NIH HHS/United States
- AI032853/AI/NIAID NIH HHS/United States
- AI027661/AI/NIAID NIH HHS/United States
- U01 AI046370/AI/NIAID NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- P30 AI073961/AI/NIAID NIH HHS/United States
- RR-024996/RR/NCRR NIH HHS/United States
- UM1 AI069474/AI/NIAID NIH HHS/United States
- AI069470/AI/NIAID NIH HHS/United States
- U01 AI034853/AI/NIAID NIH HHS/United States
- AI069494-03S1/AI/NIAID NIH HHS/United States
- UM1 AI069452/AI/NIAID NIH HHS/United States
- AI 69432/AI/NIAID NIH HHS/United States
- AI069424/AI/NIAID NIH HHS/United States
- U01 AI069415/AI/NIAID NIH HHS/United States
- UL1 RR024160/RR/NCRR NIH HHS/United States
- U01 AI069495/AI/NIAID NIH HHS/United States
- UM1 AI069556/AI/NIAID NIH HHS/United States
- U01 AI027675/AI/NIAID NIH HHS/United States
- AI027675/AI/NIAID NIH HHS/United States
- U01 AI069511/AI/NIAID NIH HHS/United States
- RR025747/RR/NCRR NIH HHS/United States
- RR024156/RR/NCRR NIH HHS/United States
- AI069418/AI/NIAID NIH HHS/United States
- U01 AI025859/AI/NIAID NIH HHS/United States
- UM1 AI069450/AI/NIAID NIH HHS/United States
- AI69450/AI/NIAID NIH HHS/United States
- UL1 RR025747/RR/NCRR NIH HHS/United States
- UM1 AI069532/AI/NIAID NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
- U01 AI032782/AI/NIAID NIH HHS/United States
- U01 AI069424/AI/NIAID NIH HHS/United States
- AI050409/AI/NIAID NIH HHS/United States
- AI045008/AI/NIAID NIH HHS/United States
- AI-069513/AI/NIAID NIH HHS/United States
- AI-069467/AI/NIAID NIH HHS/United States
- AI069472/AI/NIAID NIH HHS/United States
- UM1 AI069419/AI/NIAID NIH HHS/United States
- RR025780/RR/NCRR NIH HHS/United States
- AI50410/AI/NIAID NIH HHS/United States
- U01 AI069419/AI/NIAID NIH HHS/United States
- UM1 AI069511/AI/NIAID NIH HHS/United States
- U01 AI069494/AI/NIAID NIH HHS/United States
- U01 AI069452/AI/NIAID NIH HHS/United States
- UM1 AI069467/AI/NIAID NIH HHS/United States
- U01 AI027665/AI/NIAID NIH HHS/United States
- AI069477/AI/NIAID NIH HHS/United States
- RR00046/RR/NCRR NIH HHS/United States
- AI069471/AI/NIAID NIH HHS/United States
- U01 AI069471/AI/NIAID NIH HHS/United States
- U01 AI069472/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- AI025859/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- UM1 AI069418/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials