

Computer decision support software safely improves glycemic control in the burn intensive care unit: a randomized controlled clinical study
- PMID: 21240001
- PMCID: PMC3042492
- DOI: 10.1097/BCR.0b013e31820aaebf
Computer decision support software safely improves glycemic control in the burn intensive care unit: a randomized controlled clinical study
Abstract
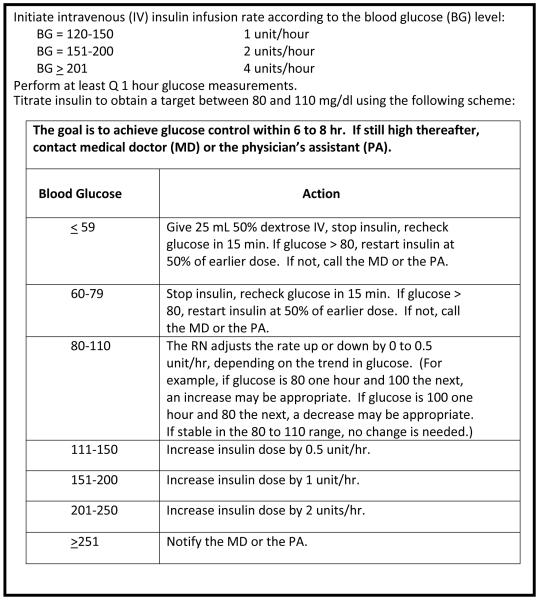
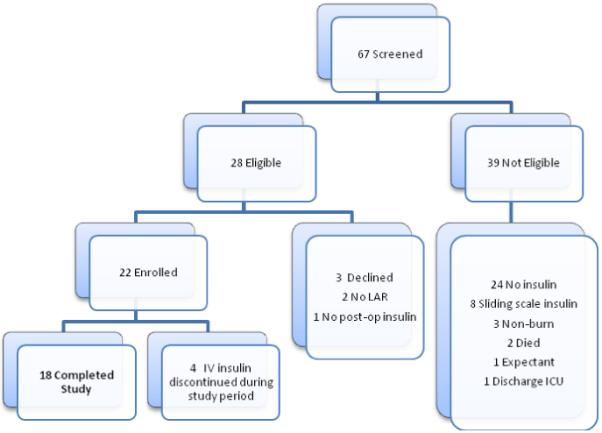
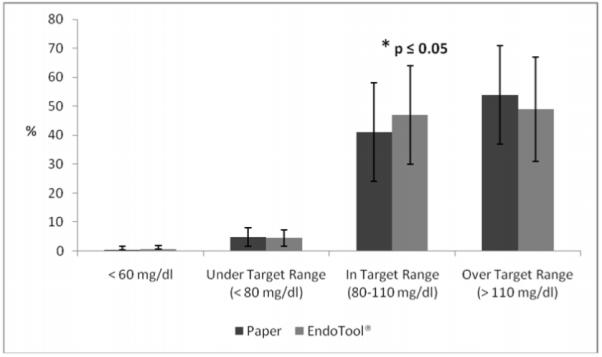
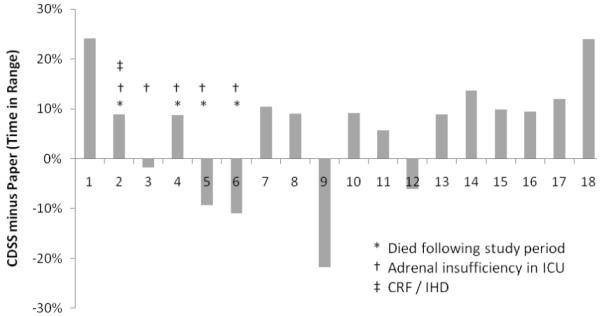
The optimal method for glycemic control in the critically burned patient is unknown. The purpose of this randomized controlled study was to determine the safety and efficacy of computer decision support software (CDSS) to control serum glucose concentration in a burn intensive care unit. Eighteen adult burn/trauma patients receiving continuous insulin infusion were initially randomized to receive glucose management by a traditional paper protocol or a computer protocol (CP) for 72 hours and then crossed over to the alternate method for an additional 72 hours. Time in target glucose range (range: 80-110 mg/dl) was higher in the CP group (47 ± 17% vs 41 ± 16.6%; P ≤ .05); time over target range was not significantly reduced in the CP group (49 ± 17.8% vs 54 ± 17.1%; P = .08); and no difference was noted in time under target range of 80 mg/dl (CP: 4.5 ± 2.8%, paper protocol: 4.8 ± 3.3%; P = .8), less than 60 mg/dl (P = .7), and less than 40 mg/dl (P = 1.0). Severe hypoglycemic events (<40 mg/dl) did not differ from the CP group compared with historical controls for patients receiving no insulin (P = .6). More glucose measurements were performed in the CP group (P = .0003), and nursing staff compliance with CP recommendations was greater (P < .0001). Glycemic control using CDSS is safe and effective for the critically burned patient. Time in target range improved without increase in hypoglycemic events. CDSS enhanced consistency in practice, providing standardization among nursing staff.
Figures
References
-
- Pham TN, Warren AJ, Pham HH, et al. Impact of tight glycemic control in severely burned children. J Trauma. 2005;59:1148–1154. - PubMed
-
- Mowlavi A, Andrews K, Milner S, et al. The effects of hyperglycemia on skin graft survival in the burn patient. Ann Plast Surg. 2000;45:629–632. - PubMed
-
- Gore DC, Chinkes DL, Hart DW, et al. Hyperglycemia exacerbates muscle protein catabolism in burn-injured patients. Crit Care Med. 2002;30:2438–2442. - PubMed
-
- Gore DC, Chinkes D, Heggers J, et al. Association of hyperglycemia with increased mortality after severe burn injury. J Trauma. 2001;51:540–544. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
