

Clinical cartilage restoration: evolution and overview
- PMID: 21240578
- PMCID: PMC3171560
- DOI: 10.1007/s11999-010-1764-z
Clinical cartilage restoration: evolution and overview
Abstract
Background: Clinical cartilage restoration is evolving, with established and emerging technologies. Randomized, prospective studies with adequate power comparing the myriad of surgical techniques used to treat chondral injuries are still lacking and it remains a challenge for the surgeon treating patients to make evidence-based decisions.
Questions/purposes: We reviewed the history of the major cartilage repair/restorative procedures, indications for currently available repair/restorative procedures, and postoperative management.
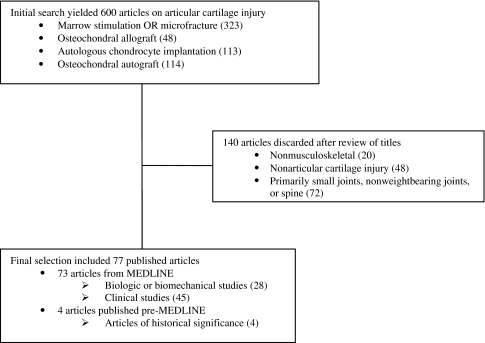
Methods: We performed searches using MEDLINE and cartilage-specific key words to identify all English-language literature. Articles were selected based on their contributions to our current understanding of the basic science and clinical treatment of articular cartilage lesions or historical importance. We then selected 77 articles, two of which are articles of historical importance.
Results: Current cartilage restorative techniques include débridement, microfracture, osteochondral fragment repair, osteochondral allograft, osteochondral autograft, and autologous chondrocyte transplantation. Pending techniques include two-staged cell-based therapies integrated into a variety of scaffolds, single-stage cell-based therapy, and augmentation of marrow stimulation, each with suggested indications including lesion size, location, and activity demands of the patient. The literature demonstrates variable improvements in pain and function contingent upon multiple variables including indications and application.
Conclusions: For the patient with symptomatic chondral injury, numerous techniques are available to the surgeon to relieve pain and improve function. Until rigorous clinical trials (prospective, adequately powered, randomized control) are available, treatment decisions should be guided by expert extrapolation of the available literature based in historically sound principles.
Figures
References
-
- Ahmad CS, Cohen ZA, Levine WN, Ateshian GA, Mow VC. Biomechanical and topographic considerations for autologous osteochondral grafting in the knee. Am J Sports Med. 2001;29:201–206. - PubMed
-
- Bobic V, Morgan C, Carter T. Osteochondral autologous graft transfer. Oper Tech Sports Med. 2000;8:168–178. doi: 10.1053/otsm.2000.7506. - DOI
-
- Brittberg M, Peterson L. Introduction to an articular cartilage classification. ICRS Newsletter. 1998;1:5–8.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
