

Value of MRI and diffusion-weighted MRI for the diagnosis of locally recurrent rectal cancer
- PMID: 21240647
- PMCID: PMC3088810
- DOI: 10.1007/s00330-010-2052-8
Value of MRI and diffusion-weighted MRI for the diagnosis of locally recurrent rectal cancer
Abstract
Objectives: To evaluate the accuracy of standard MRI, diffusion-weighted MRI (DWI) and fusion images for the diagnosis of locally recurrent rectal cancer in patients with a clinical suspicion of recurrence.
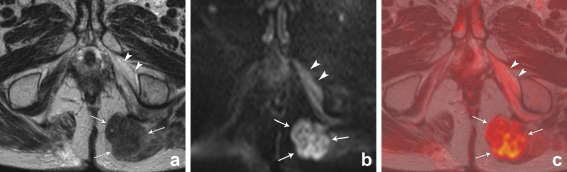
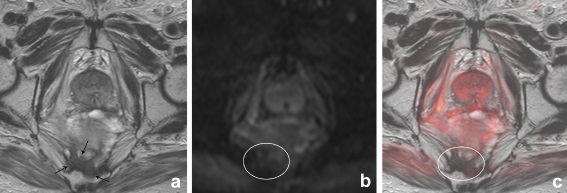
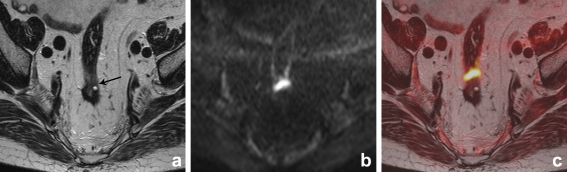
Methods: Forty-two patients with a clinical suspicion of recurrence underwent 1.5-T MRI consisting of standard T2-weighted FSE (3 planes) and an axial DWI (b0,500,1000). Two readers (R1,R2) independently scored the likelihood of recurrence; [1] on standard MRI, [2] on standard MRI+DWI, and [3] on T2-weighted+DWI fusion images.
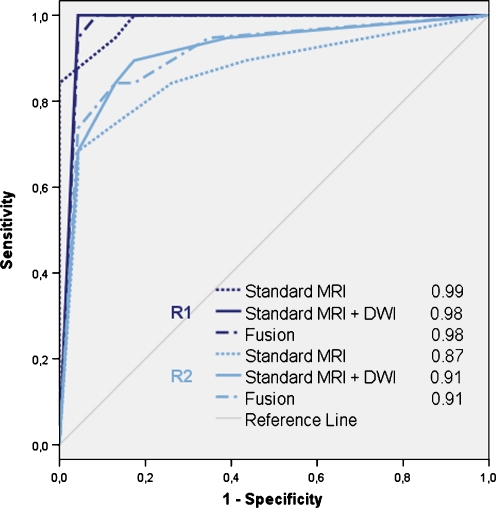
Results: 19/42 patients had a local recurrence. R1 achieved an area under the ROC-curve (AUC) of 0.99, sensitivity 100% and specificity 83% on standard MRI versus 0.98, 100% and 91% after addition of DWI (p = 0.78). For R2 these figures were 0.87, 84% and 74% on standard MRI and 0.91, 89% and 83% with DWI (p = 0.09). Fusion images did not significantly improve the performance. Interobserver agreement was κ0.69 for standard MRI, κ0.82 for standard MRI+DWI and κ0.84 for the fusion images.
Conclusions: MRI is accurate for the diagnosis of locally recurrent rectal cancer in patients with a clinical suspicion of recurrence. Addition of DWI does not significantly improve its performance. However, with DWI specificity and interobserver agreement increase. Fusion images do not improve accuracy.
Figures
References
-
- Jeffery M, Hickey BE, Hider PN. Follow-up strategies for patients treated for non-metastatic colorectal cancer. Cochrane Database Syst Rev. 2007;24:CD002200. - PubMed
-
- Kusters M, Marijnen CA, van de Velde CJ, Rutten HJ, Lahaye MJ, Kim JH, Beets-Tan RG, Beets GL. Patterns of local recurrence in rectal cancer; a study of the Dutch TME trial. Eur J Surg Oncol. 2010;36:470–476. - PubMed
-
- Desch CE, Benson AB, 3rd, Somerfield MR, Flynn PJ, Krause C, Loprinzi CL, Minsky BD, Pfister DG, Virgo KS, Petrelli NJ, American Society of Clinical Oncology Colorectal cancer surveillance: 2005 update of an American society of clinical oncology practice guideline. J Clin Oncol. 2005;23:8512–8519. doi: 10.1200/JCO.2005.04.0063. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
