

Management of delayed major visceral arterial bleeding after pancreatic surgery
- PMID: 21241431
- PMCID: PMC3044348
- DOI: 10.1111/j.1477-2574.2010.00260.x
Management of delayed major visceral arterial bleeding after pancreatic surgery
Abstract
Objectives: Postoperative bleeding represents a life-threatening complication after pancreatic surgery. Recent developments in interventional radiology have challenged the role of surgery in bleeding control. This study aimed to assess the management of major haemorrhagic complications after pancreatic surgery at a tertiary referral centre.
Methods: Between August 1998 and June 2009, 18 patients with major bleeding after pancreatic surgery were admitted to the University Hospital of Zurich, Zurich, Switzerland. We retrospectively analysed their medical charts, focusing on diagnosis, therapy and outcome.
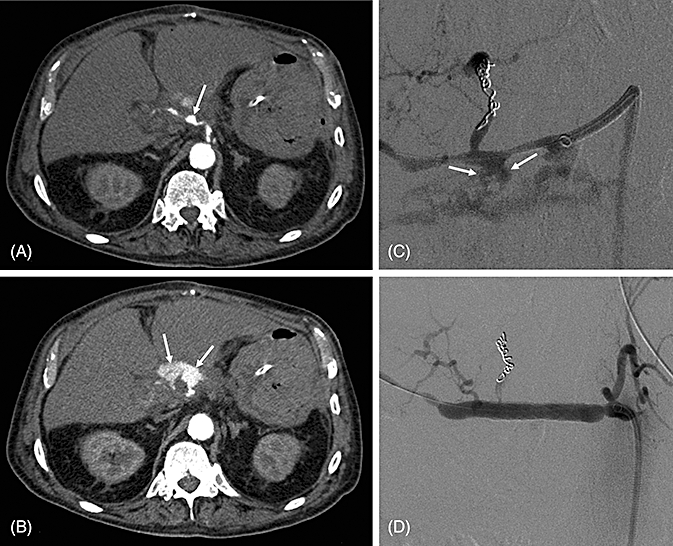
Results: Major arterial bleeding occurred after a median postoperative interval of 21.5 days (range: 9-259 days). Seventeen patients demonstrated various symptoms, such as repeated upper gastrointestinal bleeding or haemorrhagic shock. Diagnosis was usually made by contrast-enhanced computed tomography (CT). Leakage of the pancreaticojejunostomy caused the formation of a pseudoaneurysm in 78% of patients. Haemostasis was achieved in 10 patients by interventional radiology. Two patients died of massive re-bleeding. Six patients underwent primary emergency surgery, which five did not survive.
Conclusions: Delayed bleeding after pancreatic surgery is suspicious for a pseudoaneurysm. Contrast-enhanced CT followed by early angiography provides accurate diagnosis and treatment. Interventional radiological treatment should be preferred over primary surgery because it is currently the most life-saving approach.
© 2011 International Hepato-Pancreato-Biliary Association.
Figures

References
-
- de Castro SMM, Busch ORC, Gouma DJ. Management of bleeding and leakage after pancreatic surgery. Best Pract Res Clin Gastroenterol. 2004;18:847–864. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
