

Stage II palliation of hypoplastic left heart syndrome without cardiopulmonary bypass
- PMID: 21241860
- PMCID: PMC5253184
- DOI: 10.1016/j.jtcvs.2010.10.047
Stage II palliation of hypoplastic left heart syndrome without cardiopulmonary bypass
Abstract
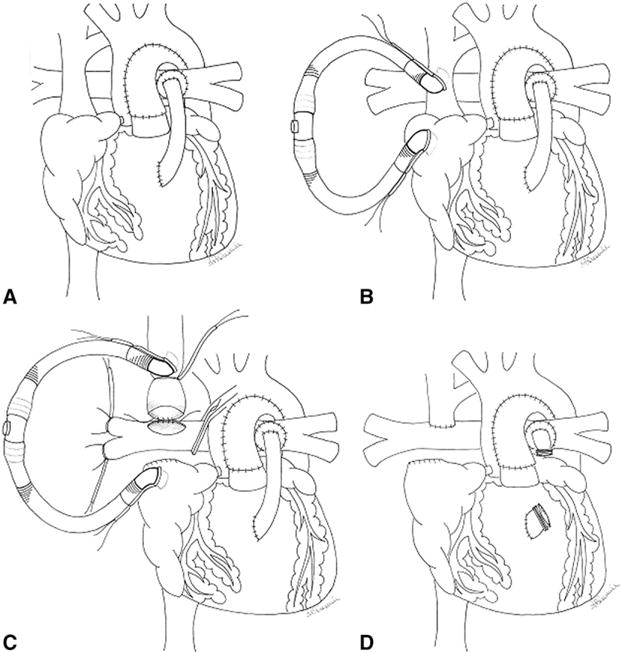
Objectives: Bidirectional cavopulmonary anastomosis has been performed without cardiopulmonary bypass for some single-ventricle heart defects. Limited data are available for the outcomes of off-pump bidirectional cavopulmonary anastomosis in infants with hypoplastic left heart syndrome. The purpose of this study is to determine the early outcomes for stage II palliation of hypoplastic left heart syndrome without cardiopulmonary bypass.
Methods: This is a retrospective review of infants having surgical palliation of hypoplastic left heart syndrome from April 2003 to March 2010 at a single institution.
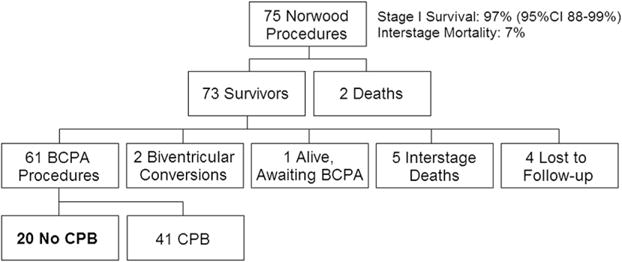
Results: Seventy-five infants had a modified Norwood procedure, 65 with a right ventricle-pulmonary artery conduit, 10 with an aortopulmonary shunt, 2 with atrioventricular valve repair, and 3 with extracorporeal life support. Sixty-eight patients had hypoplastic left heart syndrome or one of its variants, and 7 had other single-ventricle lesions. There were 2 stage I deaths. Stage I survival was 97% (95% confidence interval, 88%-99%). Another 5 infants succumbed in the interstage period. Of the 68 stage I and interstage survivors, 61 had bidirectional cavopulmonary anastomoses, 20 without cardiopulmonary bypass. Median age was 6 months (range, 4-13 months), and median weight was 6.1 kg (range, 5.2-9.0 kg). There were no conversions to cardiopulmonary bypass when off-pump bidirectional cavopulmonary anastomosis was attempted. There were no hospital deaths. Median ventilation duration was 10 hours (range, 6-18 hours), and length of stay was 5 days (range, 4-9 days). Follow-up was available on all infants at a median duration of 17 months (range, 3-43 months), with no unplanned reinterventions.
Conclusions: Bidirectional cavopulmonary anastomosis without the use of cardiopulmonary bypass can be performed safely and with low mortality for selected infants with hypoplastic left heart syndrome. Midterm to long-term outcomes remain to be determined.
Copyright © 2011 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Karl TR. The bidirectional cavopulmonary shunt for hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2001;4:58–70. - PubMed
-
- Jaquiss RD, Ghanayem NS, Hoffman GM, Fedderly RT, Cava JR, Mussatto KA, et al. Early cavopulmonary anastomosis in very young infants after the Norwood procedure: impact on oxygenation, resource utilization, and mortality. J Thorac Cardiovasc Surg. 2004;127:982–9. - PubMed
-
- Scheurer MA, Hill EG, Vasuki N, Maurer S, Graham EM, Bandisode V, et al. Survival after bidirectional cavopulmonary anastomosis: analysis of preoperative risk factors. J Thorac Cardiovasc Surg. 2007;134:82–9. e1–2. - PubMed
-
- Lamberti JJ, Spicer RL, Waldman JD, Grehl TM, Thomson D, George L, et al. The bidirectional cavopulmonary shunt. J Thorac Cardiovasc Surg. 1990;100:22–30. - PubMed
-
- Luo XJ, Yan J, Wu QY, Yang KM, Xu JP, Liu YL. Clinical application of bidirectional Glenn shunt with off-pump technique. Asian Cardiovasc Thorac Ann. 2004;12:103–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
