

Possible geographical barriers to trauma center access for vulnerable patients in the United States: an analysis of urban and rural communities
- PMID: 21242445
- PMCID: PMC3121679
- DOI: 10.1001/archsurg.2010.299
Possible geographical barriers to trauma center access for vulnerable patients in the United States: an analysis of urban and rural communities
Abstract
Objective: To study whether traditionally vulnerable populations have worse geographic access to trauma centers.
Design: A cross-sectional analysis using data from the American Hospital Association Annual Survey from 2005 linked with zip code-level data from the US Census. We used a multinomial logit model to examine the odds of having difficult as opposed to easy access to trauma centers for a given subgroup of vulnerable populations.
Setting and participants: Population in rural and urban communities as defined by zip codes in the United States.
Main outcome measures: Each community's distance to the nearest trauma center (levels I-III).
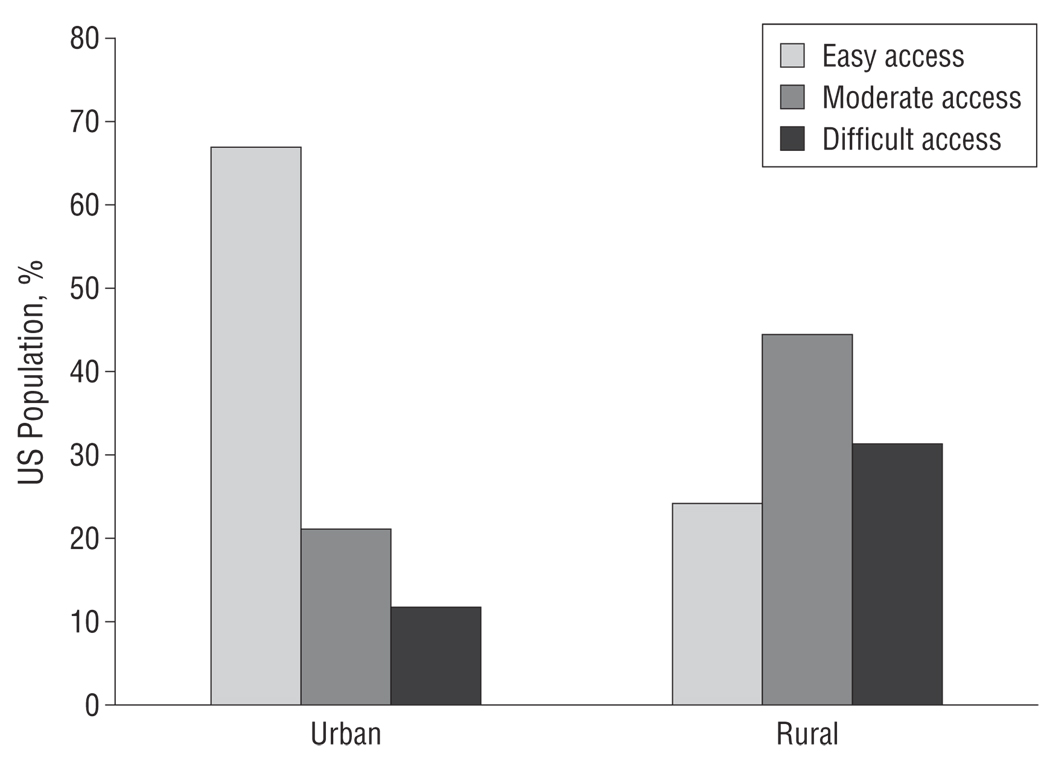
Results: In urban areas, 67% of the population had easy access to trauma centers and 12% had difficult access compared with 24% and 31% in rural areas, respectively. Areas with higher shares of the following vulnerable population groups had higher risks (odds ratios) of facing difficult access to trauma center services in 2005: foreign born in urban areas (1.65 for a medium share and 2.18 for a high share [both P < .01]); African American in urban and rural areas (1.25 for a medium share and 1.35 for a high share, respectively [both P < .05]); and near-poor in urban and rural areas (1.52 [P < .05] and 1.69 [P < .01] for a high share, respectively).
Conclusions: A significant segment of the US population (representing 38.4 million people) does not have access to trauma care within 1 hour of driving time. Moreover, certain vulnerable groups are at higher risk than others for worse access to trauma centers. Stakeholders and health care planners should consider these factors in the development of trauma systems because a mismatch of potential need and access could signal inefficiencies in the delivery of care.
Figures
Comment in
-
Disparities in access to care: Does it translate into worse outcomes?: Comment on "Possible geographical barriers to trauma center access for vulnerable patients in the United States".Arch Surg. 2011 Jan;146(1):52. doi: 10.1001/archsurg.2010.301. Arch Surg. 2011. PMID: 21305710 No abstract available.
References
-
- Hulka F, Mullins RJ, Mann NC, et al. Influence of a statewide trauma system on pediatric hospitalization and outcome. J Trauma. 1997;42(3):514–519. - PubMed
-
- DeMaria EJ, Kenney PR, Merriam MA, Casanova LA, Gann DS. Aggressive trauma care benefits the elderly. J Trauma. 1987;27(11):1200–1206. - PubMed
-
- MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366–378. - PubMed
-
- Bazzoli GJ, Kang R, Hasnain-Wynia R, Lindrooth RC. An update on safety-net hospitals: coping with the late 1990s and early 2000s. Health Aff (Millwood) 2005;24(4):1047–1056. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
