

A2B adenosine receptor blockade enhances macrophage-mediated bacterial phagocytosis and improves polymicrobial sepsis survival in mice
- PMID: 21242513
- PMCID: PMC3708265
- DOI: 10.4049/jimmunol.1001567
A2B adenosine receptor blockade enhances macrophage-mediated bacterial phagocytosis and improves polymicrobial sepsis survival in mice
Abstract
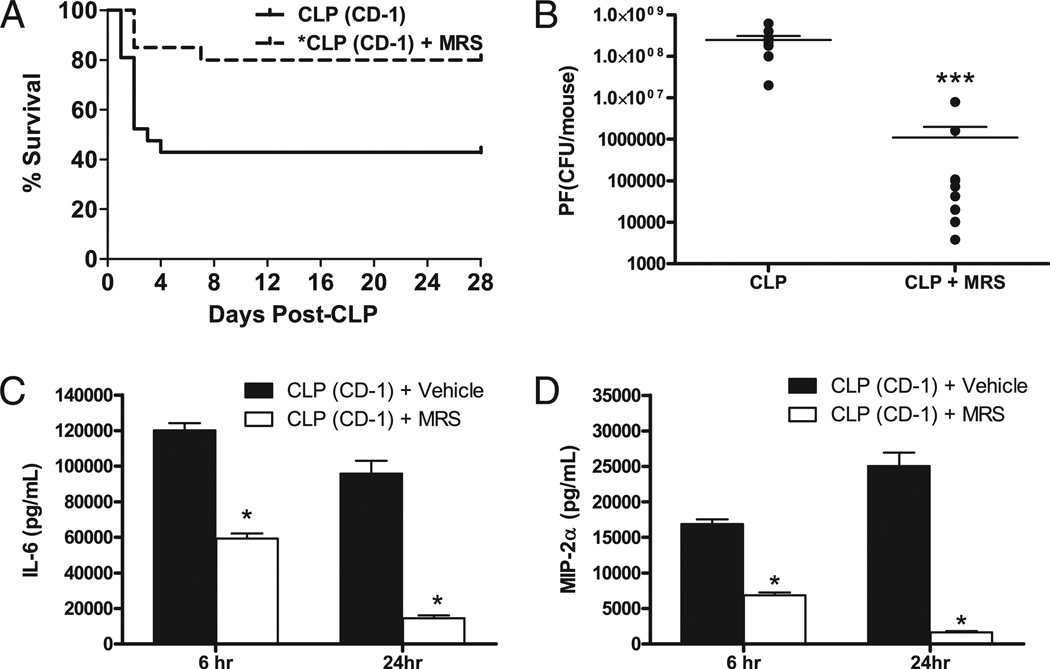
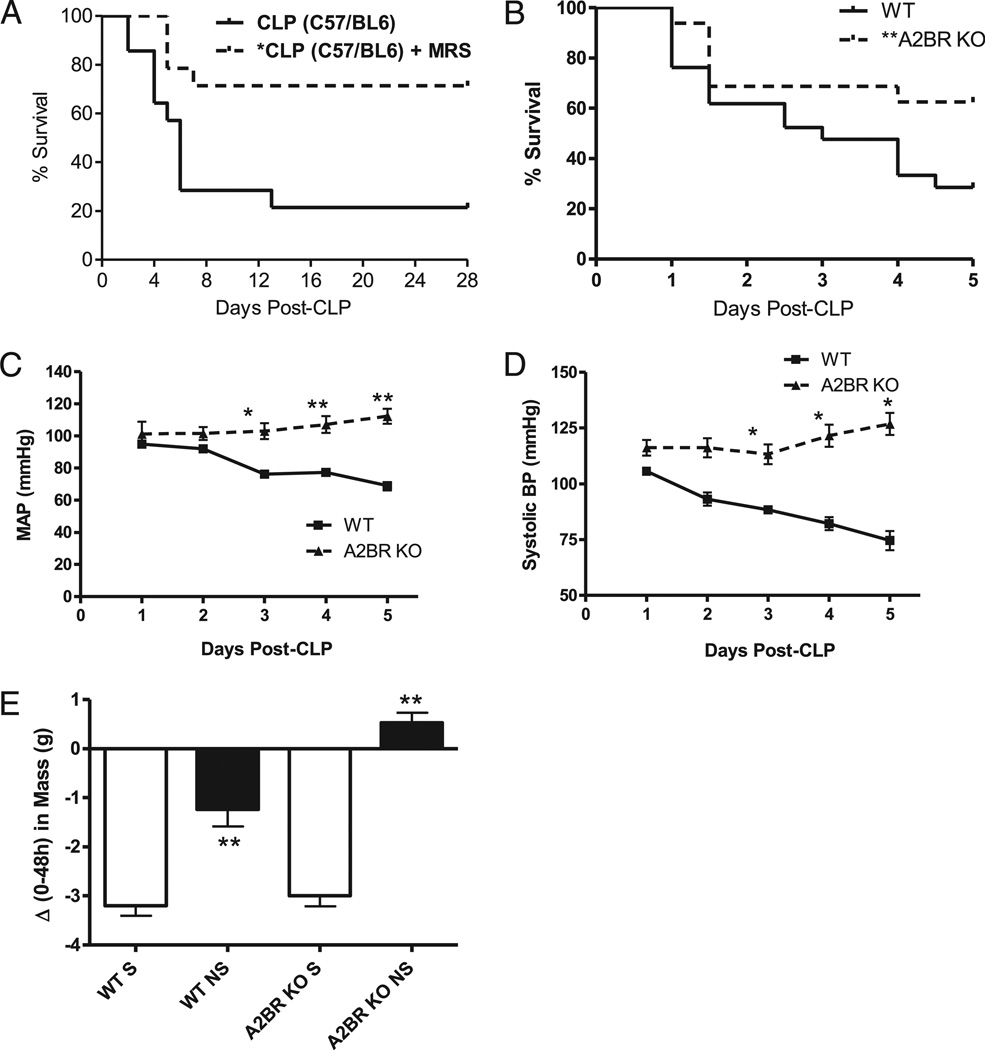
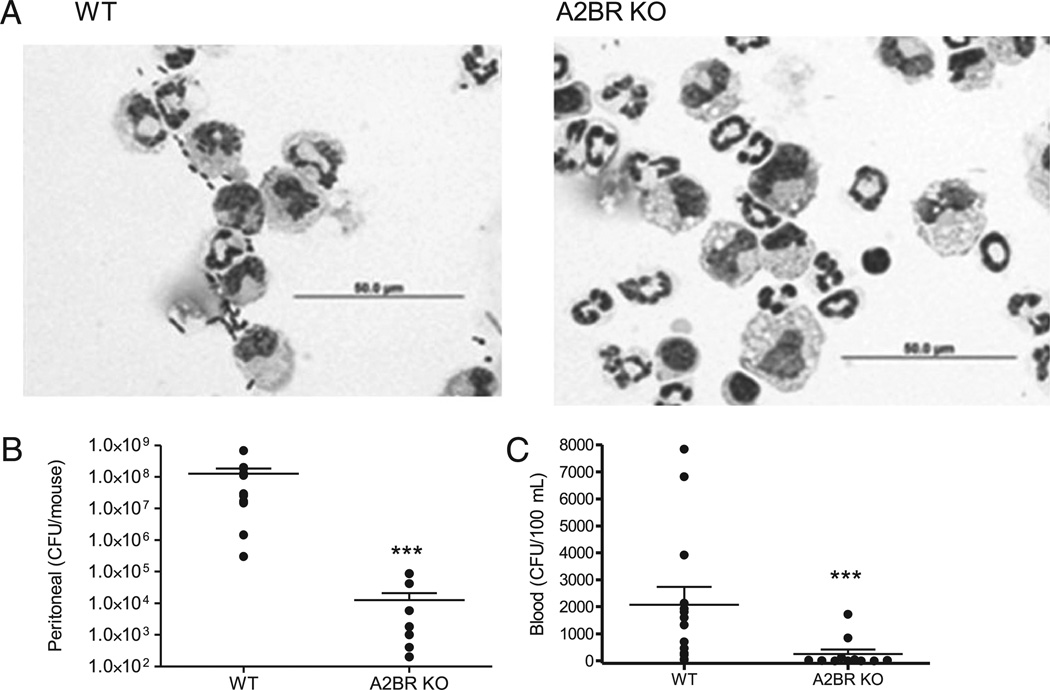
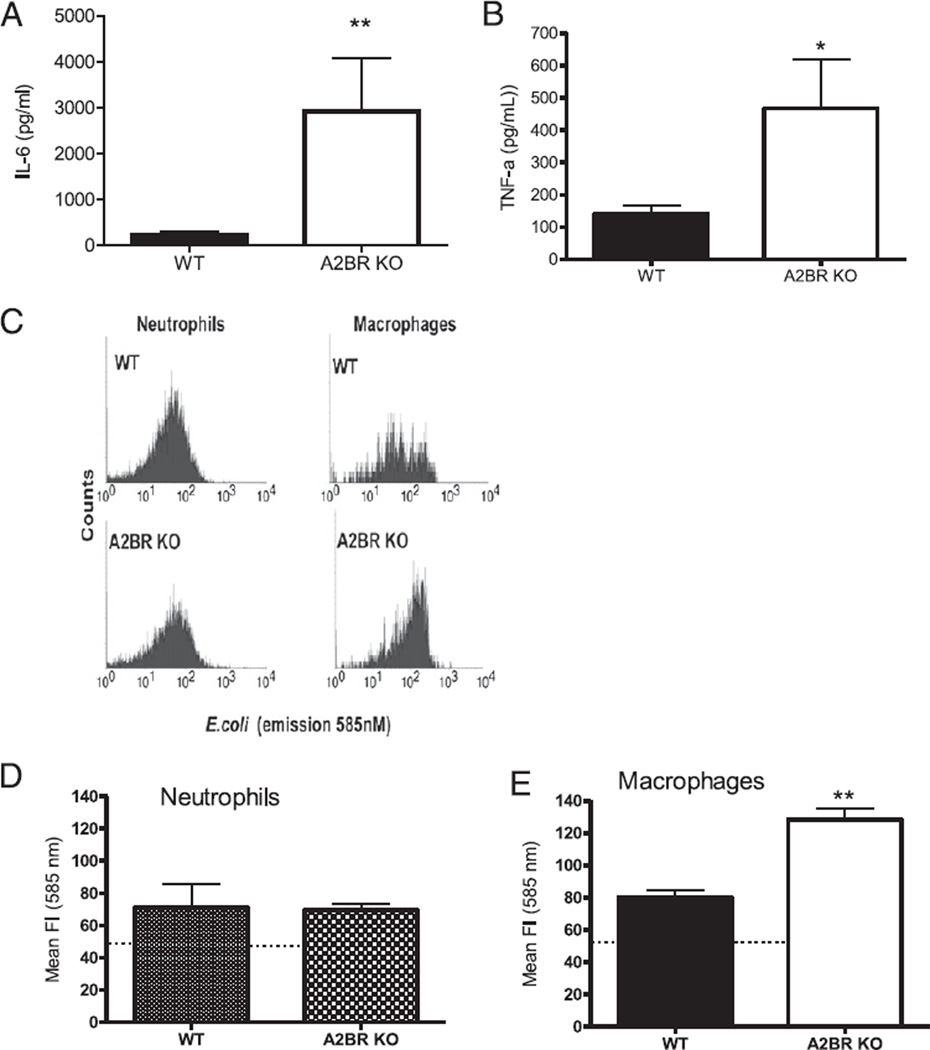
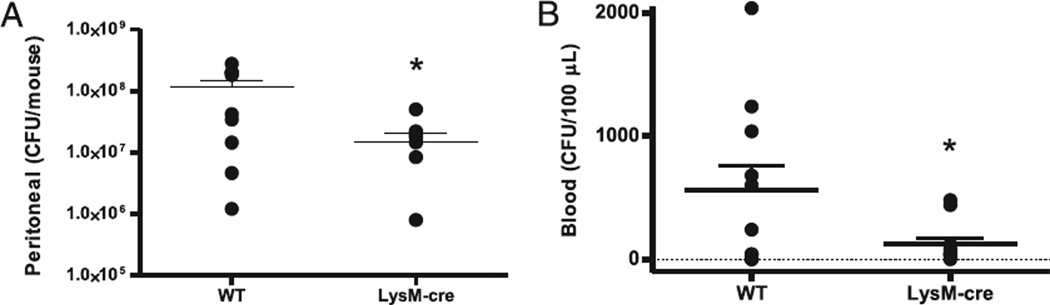
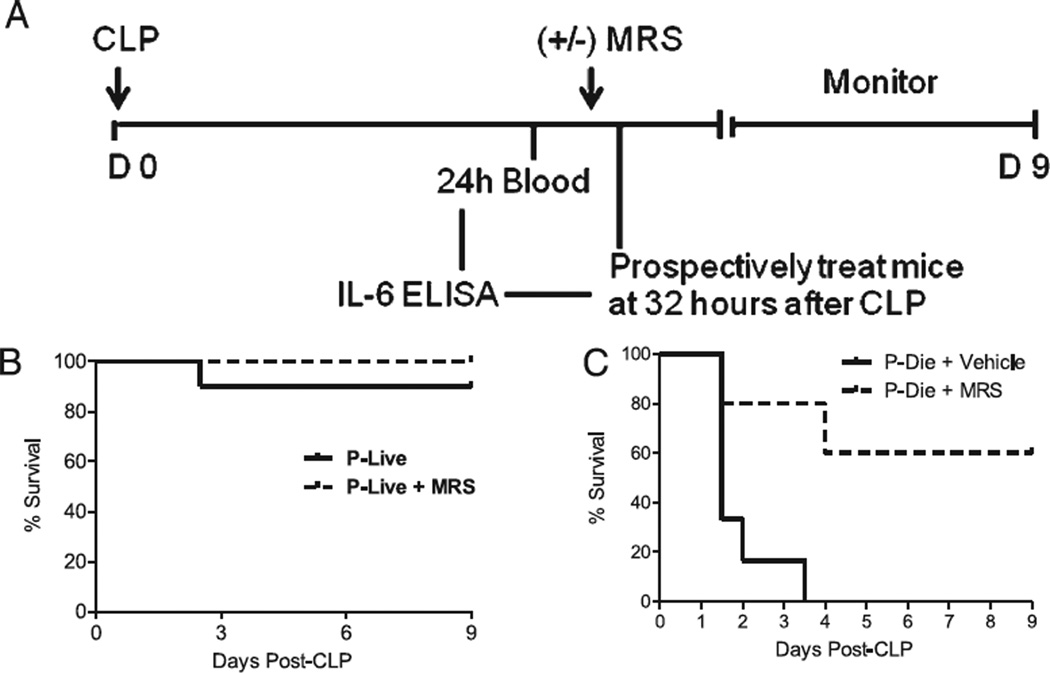
Antimicrobial treatment strategies must improve to reduce the high mortality rates in septic patients. In noninfectious models of acute inflammation, activation of A2B adenosine receptors (A2BR) in extracellular adenosine-rich microenvironments causes immunosuppression. We examined A2BR in antibacterial responses in the cecal ligation and puncture (CLP) model of sepsis. Antagonism of A2BR significantly increased survival, enhanced bacterial phagocytosis, and decreased IL-6 and MIP-2 (a CXC chemokine) levels after CLP in outbred (ICR/CD-1) mice. During the CLP-induced septic response in A2BR knockout mice, hemodynamic parameters were improved compared with wild-type mice in addition to better survival and decreased plasma IL-6 levels. A2BR deficiency resulted in a dramatic 4-log reduction in peritoneal bacteria. The mechanism of these improvements was due to enhanced macrophage phagocytic activity without augmenting neutrophil phagocytosis of bacteria. Following ex vivo LPS stimulation, septic macrophages from A2BR knockout mice had increased IL-6 and TNF-α secretion compared with wild-type mice. A therapeutic intervention with A2BR blockade was studied by using a plasma biomarker to direct therapy to those mice predicted to die. Pharmacological blockade of A2BR even 32 h after the onset of sepsis increased survival by 65% in those mice predicted to die. Thus, even the late treatment with an A2BR antagonist significantly improved survival of mice (ICR/CD-1) that were otherwise determined to die according to plasma IL-6 levels. Our findings of enhanced bacterial clearance and host survival suggest that antagonism of A2BRs offers a therapeutic target to improve macrophage function in a late treatment protocol that improves sepsis survival.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Bernard GR, Margolis BD, Shanies HM, Ely EW, Wheeler AP, Levy H, Wong K, Wright TJ Extended Evaluation of Recombinant Human Activated Protein C United States Investigators. Extended evaluation of recombinant human activated protein C United States Trial (ENHANCE US): a single-arm, phase 3B, multicenter study of drotrecogin alfa (activated) in severe sepsis . Chest. 2004;125:2206–2216. - PubMed
-
- Laterre PF, Levy H, Clermont G, Ball DE, Garg R, Nelson DR, Dhainaut JF, Angus DC. Hospital mortality and resource use in subgroups of the Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) trial. Crit. Care Med. 2004;32:2207–2218. - PubMed
-
- Buras JA, Holzmann B, Sitkovsky M. Animal models of sepsis: setting the stage. Nat. Rev. Drug Discov. 2005;4:854–865. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
