

Impact of EHR-based clinical decision support on adherence to guidelines for patients on NSAIDs: a randomized controlled trial
- PMID: 21242557
- PMCID: PMC3022041
- DOI: 10.1370/afm.1172
Impact of EHR-based clinical decision support on adherence to guidelines for patients on NSAIDs: a randomized controlled trial
Abstract
Purpose: Electronic health records (EHRs) with clinical decision support hold promise for improving quality of care, but their impact on management of chronic conditions has been mixed. This study examined the impact of EHR-based clinical decision support on adherence to guidelines for reducing gastrointestinal complications in primary care patients on nonsteroidal anti-inflammatory drugs (NSAIDs).
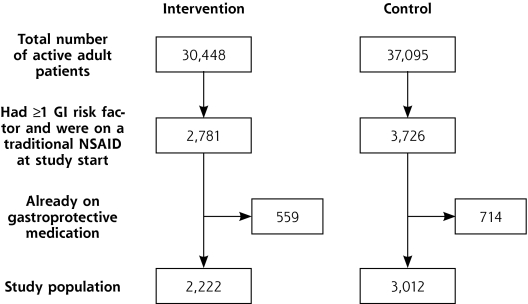
Methods: This randomized controlled trial was conducted in a national network of primary care offices using an EHR and focused on patients taking traditional NSAIDs who had factors associated with a high risk for gastrointestinal complications (a history of peptic ulcer disease; concomitant use of anticoagulants, anti-platelet medications [including aspirin], or corticosteroids; or an age of 75 years or older). The offices were randomized to receive EHR-based guidelines and alerts for high-risk patients on NSAIDs, or usual care. The primary outcome was the proportion of patients who received guideline-concordant care during the 1-year study period (June 2007-June 2008), defined as having their traditional NSAID discontinued (including a switch to a lower-risk medication), having a gastroprotective medication coprescribed, or both.
Results: Participants included 27 offices with 119 clinicians and 5,234 high-risk patients. Intervention patients were more likely than usual care patients to receive guideline-concordant care (25.4% vs 22.4%, adjusted odds ratio = 1.19; 95% confidence interval, 1.01-1.42). For individual high-risk groups, patients on low-dose aspirin were more likely to receive guideline-concordant care with the intervention vs usual care (25.0% vs 20.8%, adjusted odds ratio = 1.30; 95% confidence interval, 1.04-1.62), but there was no significant difference for patients in other high-risk groups.
Conclusions: This study showed only a small impact of EHR-based clinical decision support for high-risk patients on NSAIDs in primary care offices. These results add to the growing literature about the complexity of EHR-based clinical decision support for improving quality of care.
References
-
- Lanza FL, Chan FKL, Quigley EMM; Practice Parameters Committee of the American College of Gastroenterology. Guidelines for prevention of NSAID-related ulcer complications. Am J Gastroenterol. 2009;104(3):728–738. - PubMed
-
- American Gastroenterological Association, Wilcox CM, Jeroan A, et al. Consensus development conference on the use of nonsteroidal anti-Inflammatory agents, including cyclooxygenase-2 enzyme inhibitors and aspirin. Clin Gastroenterol Hepatol. 2006;4(9):1082–1089. - PubMed
-
- Schnitzer TJ; American College of Rheumatology. Update of ACR guidelines for osteoarthritis: role of the coxibs. J Pain Symptom Manage. 2002;23(4 Suppl):S24–S30, discussion S31–S34. - PubMed
-
- Smalley W, Stein CM, Arbogast PG, Eisen G, Ray WA, Griffin M. Underutilization of gastroprotective measures in patients receiving nonsteroidal antiinflammatory drugs. Arthritis Rheum. 2002;46(8): 2195–2200. - PubMed
-
- Abraham NS, El-Serag HB, Johnson ML, et al. National adherence to evidence-based guidelines for the prescription of non-steroidal anti-inflammatory drugs. Gastroenterology. 2005;129(4):1171–1178. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical