

The paradox of breastfeeding-associated morbidity among late preterm infants
- PMID: 21244492
- PMCID: PMC3216635
- DOI: 10.1111/j.1552-6909.2010.01211.x
The paradox of breastfeeding-associated morbidity among late preterm infants
Abstract
Objective: To synthesize the published research pertaining to breastfeeding establishment and outcomes among late preterm infants and to describe the state of the science on breastfeeding within this population.
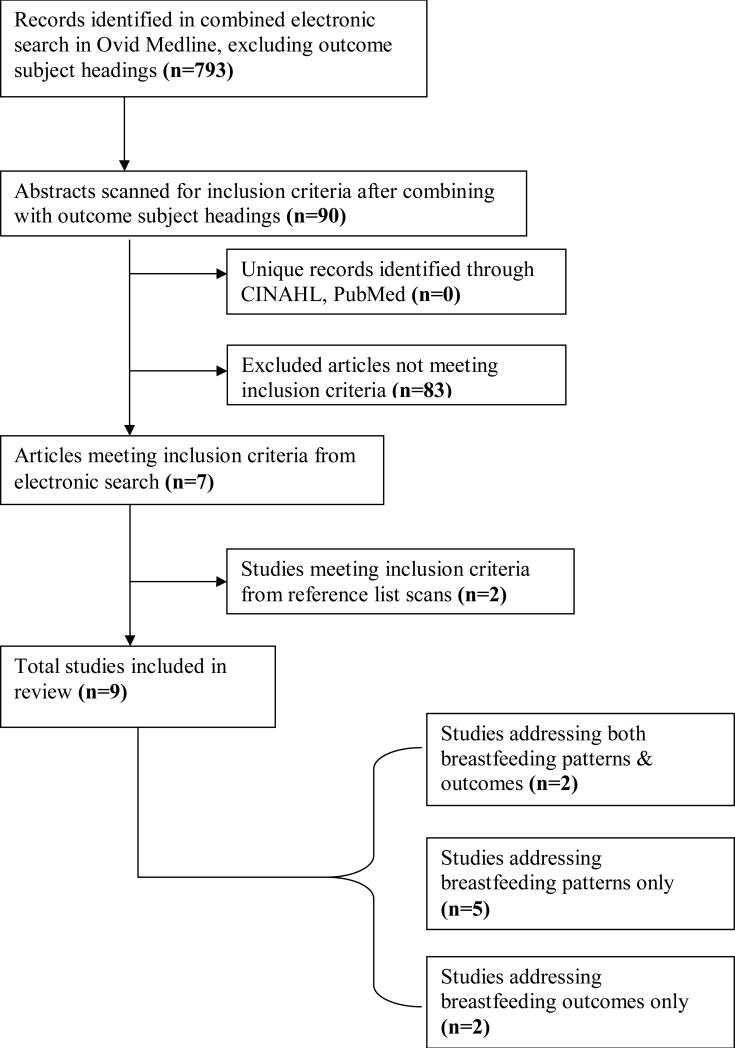
Data sources: Online databases Ovid MEDLINE, CINAHL, PubMed, and reference lists of reviewed articles.
Study selection: Nine data-based research articles examining breastfeeding patterns and outcomes among infants born between 34 0/7 and 36 6/7 weeks gestation or overlapping with this time period by at least 2 weeks.
Data extraction: Effect sizes and descriptive statistics pertaining to breastfeeding initiation, duration, exclusivity, and health outcomes among late preterm breastfed infants.
Data synthesis: Among late preterm mother/infant dyads, breastfeeding initiation appears to be approximately 59% to 70% (U.S.), whereas the odds of breastfeeding beyond 4 weeks or to the recommended 6 months (exclusive breastfeeding) appears to be significantly less than for term infants, and possibly less than infants ≤34 to 35 weeks gestation. Breastfeeding exclusivity is not routinely reported. Rehospitalization, often related to "jaundice" and "poor feeding," is nearly twice as common among late preterm breastfed infants as breastfed term or nonbreastfed late preterm infants. Barriers to optimal breastfeeding in this population are often inferred from research on younger preterm infants, and evidence-based breastfeeding guidelines are lacking.
Conclusions: Late preterm infants are at greater risk for breastfeeding-associated rehospitalization and poor breastfeeding establishment compared to their term (and possibly early preterm) counterparts. Contributing factors have yet to be investigated systematically.
© 2011 AWHONN, the Association of Women's Health, Obstetric and Neonatal Nurses.
Figures
References
-
- Adams-Chapman I. Neurodevelopmental outcome of the late preterm infant. Clinics in Perinatology. 2006;33(4):947–964. - PubMed
-
- Allen EC, Manuel JC, Legault C, Naughton MJ, Pivor C, O'Shea TM. Perception of child vulnerability among mothers of former premature infants. Pediatrics. 2004;113(2):267–273. - PubMed
-
- Altman M, Vanpe'e M, Cnattingius S, Norman M. Moderately preterm infants and determinants of length of hospital stay. Archives of Disease in Childhood - Fetal and Neonatal Edition. 2009;94:F414–F418. - PubMed
-
- Arora S, McJunkin C, Wehrer J, Kuhn P. Major factors influencing breastfeeding rates: Mother's perception of father's attitude and milk supply. Pediatrics. 2000;106(5):E67. - PubMed
-
- Ball TM, Wright AL. Health care costs of formula-feeding in the first year of life. Pediatrics. 1999;103(4 Pt 2):870–876. - PubMed
