

Revisiting the value of pre-hospital tracheal intubation: an all time systematic literature review extracting the Utstein airway core variables
- PMID: 21244667
- PMCID: PMC3222062
- DOI: 10.1186/cc9973
Revisiting the value of pre-hospital tracheal intubation: an all time systematic literature review extracting the Utstein airway core variables
Abstract
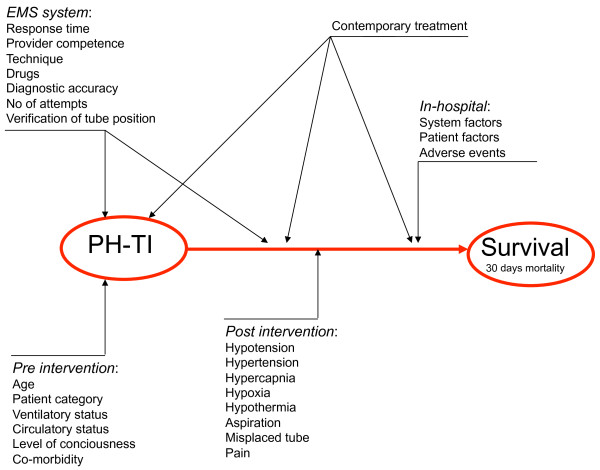
Introduction: Although tracheal intubation (TI) in the pre-hospital setting is regularly carried out by emergency medical service (EMS) providers throughout the world, its value is widely debated. Heterogeneity in procedures, providers, patients, systems and stated outcomes, and inconsistency in data reporting make scientific reports difficult to interpret and compare, and the majority are of limited quality. To hunt down what is really known about the value of pre-hospital TI, we determined the rate of reported Utstein airway variables (28 core variables and 12 fixed-system variables) found in current scientific publications on pre-hospital TI.
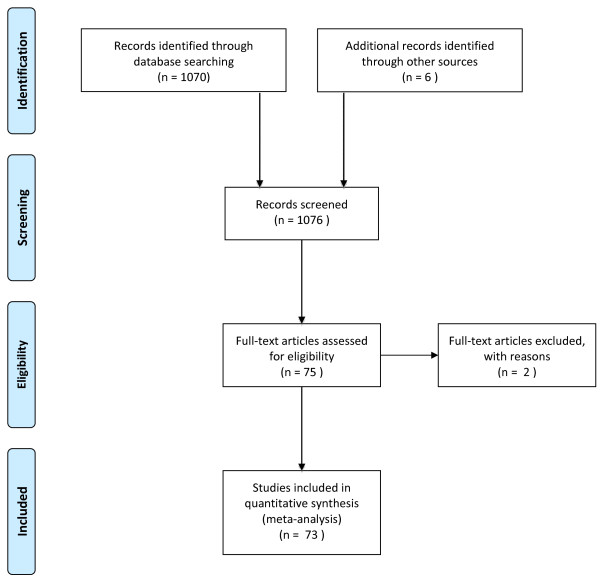
Methods: We performed an all time systematic search according to the PRISMA guidelines of Medline and EMBASE to identify original research pertaining to pre-hospital TI in adult patients.
Results: From 1,076 identified records, 73 original papers were selected. Information was extracted according to an Utstein template for data reporting from in-the-field advanced airway management. Fifty-nine studies were from North American EMS systems. Of these, 46 (78%) described services in which non-physicians conducted TI. In 12 of the 13 non-North American EMS systems, physicians performed the pre-hospital TI. Overall, two were randomised controlled trials (RCTs), and 65 were observational studies. None of the studies presented the complete set of recommended Utstein airway variables. The median number of core variables reported was 10 (max 21, min 2, IQR 8-12), and the median number of fixed system variables was 5 (max 11, min 0, IQR 4-8). Among the most frequently reported variables were "patient category" and "service mission type", reported in 86% and 71% of the studies, respectively. Among the least-reported variables were "co-morbidity" and "type of available ventilator", both reported in 2% and 1% of the studies, respectively.
Conclusions: Core data required for proper interpretation of results were frequently not recorded and reported in studies investigating TI in adults. This makes it difficult to compare scientific reports, assess their validity, and extrapolate to other EMS systems. Pre-hospital TI is a complex intervention, and terminology and study design must be improved to substantiate future evidence based clinical practice.
Figures
Comment in
-
The need for standardized data reporting for prehospital airway management.Crit Care. 2011 Mar 14;15(2):133. doi: 10.1186/cc10039. Crit Care. 2011. PMID: 21457527 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
