

Sex, race, and geographic region influence clinical outcomes following primary HIV-1 infection
- PMID: 21245157
- PMCID: PMC3071223
- DOI: 10.1093/infdis/jiq085
Sex, race, and geographic region influence clinical outcomes following primary HIV-1 infection
Abstract
Background: It is unknown whether sex and race influence clinical outcomes following primary human immunodeficiency virus type 1 (HIV-1) infection.
Methods: Data were evaluated from an observational, multicenter, primarily North American cohort of HIV-1 seroconverters.
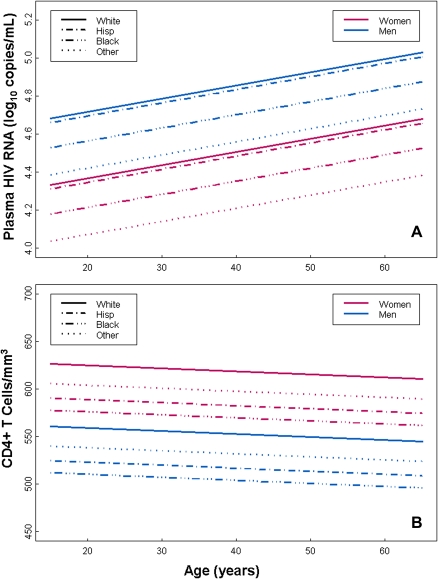
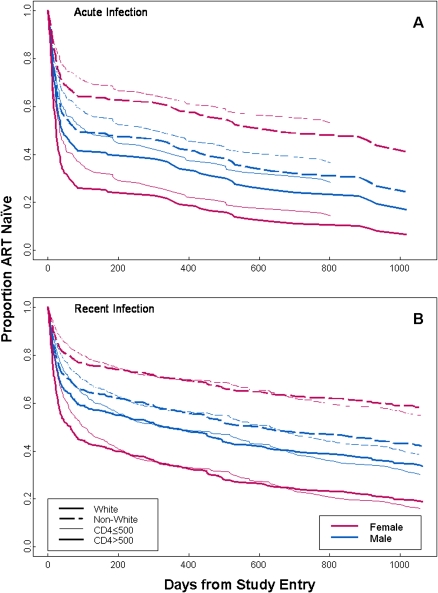
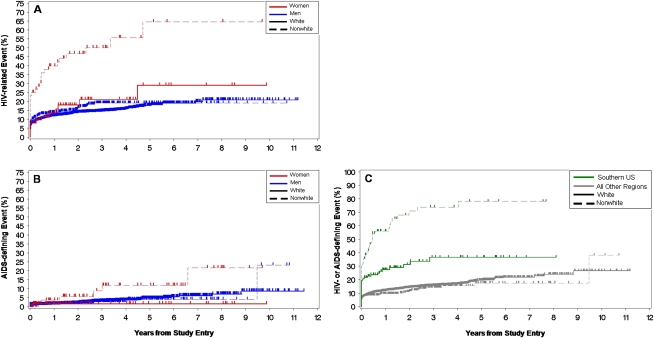
Results: Of 2277 seroconverters, 5.4% were women. At enrollment, women averaged .40 log₁₀ fewer copies/mL of HIV-1 RNA (P < .001) and 66 more CD4(+) T cells/μL (P = .006) than men, controlling for age and race. Antiretroviral therapy (ART) was less likely to be initiated at any time point by nonwhite women and men compared to white men (P < .005), and by individuals from the southern United States compared to others (P = .047). Sex and race did not affect responses to ART after 6 months (P > .73). Women were 2.17-fold more likely than men to experience >1 HIV/AIDS-related event (P < .001). Nonwhite women were most likely to experience an HIV/AIDS-related event compared to all others (P = .035), after adjusting for intravenous drug use and ART. Eight years after diagnosis, >1 HIV/AIDS-related event had occurred in 78% of nonwhites and 37% of whites from the southern United States, and 24% of whites and 17% of nonwhites from other regions (P < .001).
Conclusions: Despite more favorable clinical parameters initially, female HIV-1-seroconverters had worse outcomes than did male seroconverters. Elevated morbidity was associated with being nonwhite and residing in the southern United States.
Figures
Comment in
-
Gender, race, and geography: do they matter in primary human immunodeficiency virus infection?J Infect Dis. 2011 Feb 15;203(4):437-8. doi: 10.1093/infdis/jiq088. Epub 2011 Jan 18. J Infect Dis. 2011. PMID: 21245158 Free PMC article. No abstract available.
References
-
- Lyles RH, Munoz A, Yamashita TE, et al. Natural history of human immunodeficiency virus type 1 viremia after seroconversion and proximal to AIDS in a large cohort of homosexual men. Multicenter AIDS Cohort Study. J Infect Dis. 2000;181:872–80. - PubMed
-
- Daar ES, Little S, Pitt J, et al. Diagnosis of primary HIV-1 infection. Los Angeles County primary HIV infection recruitment network. Ann Intern Med. 2001;134:25–9. - PubMed
-
- Schacker T, Collier AC, Hughes J, Shea T, Corey L. Clinical and epidemiologic features of primary HIV infection. Ann Intern Med. 1996;125:257–64. - PubMed
-
- Sterling TR, Vlahov D, Astemborski J, Hoover DR, Margolick JB, Quinn TC. Initial plasma HIV-1 RNA levels and progression to AIDS in women and men. N Engl J Med. 2001;344:720–5. - PubMed
-
- Hubert JB RC, Boufassa F, Delfraissy JF, Meyer L. Gender, disease progression and response to HAART. Int Conf AIDS. 2002 abstract no. ThOrC1448.
Publication types
MeSH terms
Substances
Grants and funding
- AI41531/AI/NIAID NIH HHS/United States
- AI41534/AI/NIAID NIH HHS/United States
- AI41530/AI/NIAID NIH HHS/United States
- AI57005/AI/NIAID NIH HHS/United States
- AI41535/AI/NIAID NIH HHS/United States
- AI41536/AI/NIAID NIH HHS/United States
- AI41532/AI/NIAID NIH HHS/United States
- P01 AI057005/AI/NIAID NIH HHS/United States
- P01 AI055356/AI/NIAID NIH HHS/United States
- AI43638/AI/NIAID NIH HHS/United States
- R24 AI106039/AI/NIAID NIH HHS/United States
- AI43271/AI/NIAID NIH HHS/United States
- AI52403/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
