

18F-FDG PET/CT imaging in oncology
- PMID: 21245592
- PMCID: PMC3101722
- DOI: 10.4103/0256-4947.75771
18F-FDG PET/CT imaging in oncology
Abstract
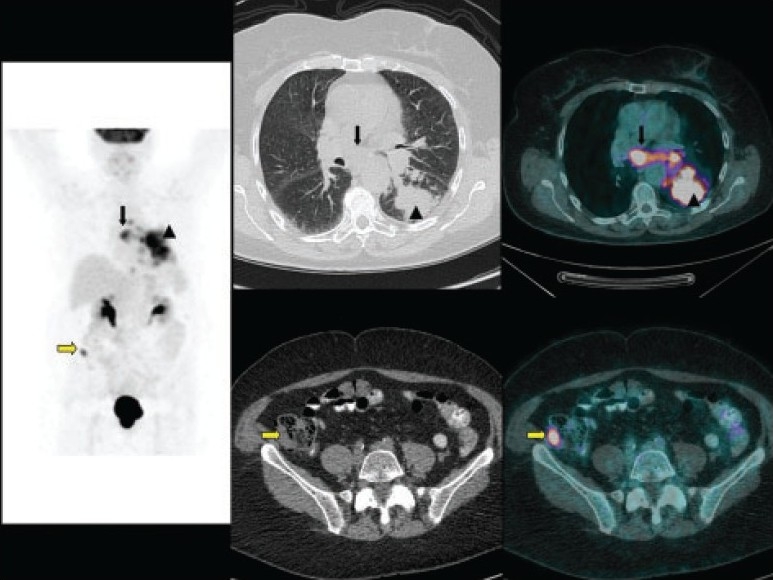
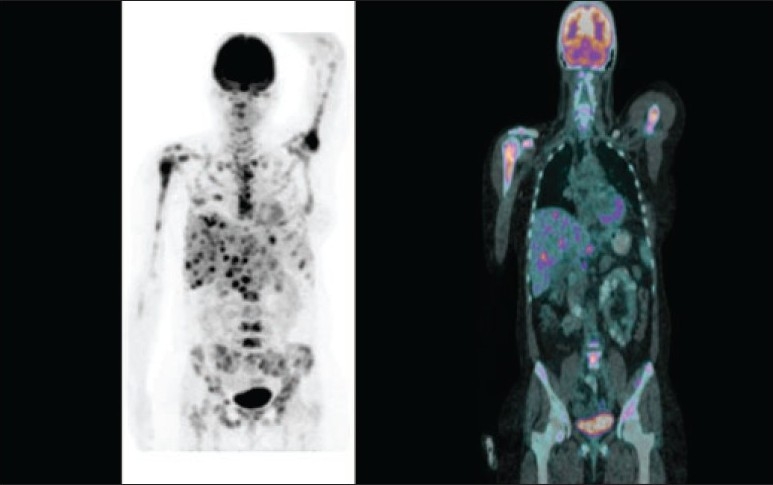
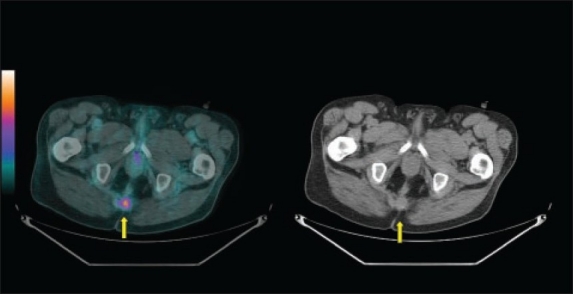
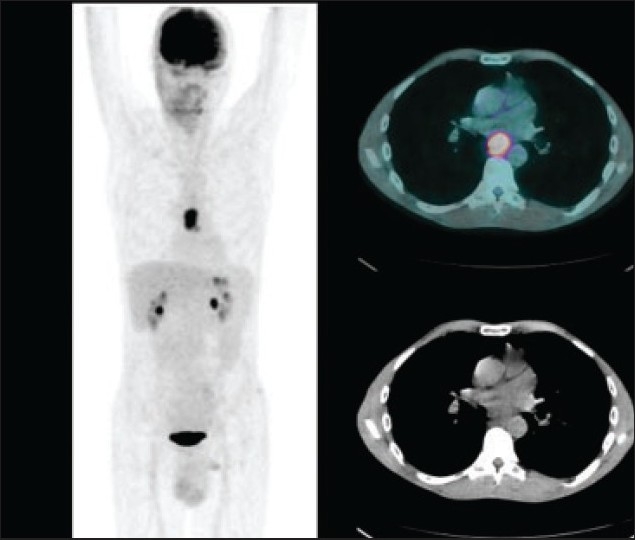
Accurate diagnosis and staging are essential for the optimal management of cancer patients. Positron emission tomography with 2-deoxy-2-[fluorine-18]fluoro-D-glucose integrated with computed tomography (18F-FDG PET/CT) has emerged as a powerful imaging tool for the detection of various cancers. The combined acquisition of PET and CT has synergistic advantages over PET or CT alone and minimizes their individual limitations. It is a valuable tool for staging and restaging of some tumors and has an important role in the detection of recurrence in asymptomatic patients with rising tumor marker levels and patients with negative or equivocal findings on conventional imaging techniques. It also allows for monitoring response to therapy and permitting timely modification of therapeutic regimens. In about 27% of the patients, the course of management is changed. This review provides guidance for oncologists/radiotherapists and clinical and surgical specialists on the use of 18F-FDG PET/CT in oncology.
Figures
References
-
- Avril N, Rosé CA, Schelling M, Dose J, Kuhn W, Bense S, et al. Breast imaging with positron emission tomography and fluorine-18 fluorodeoxyglucose: Use and limitations. J Clin Oncol. 2000;18:3495–502. - PubMed
-
- Schirrmeister H, Kühn T, Guhlmann A, Santjohanser C, Hörster T, Nüssle K, et al. Fluorine-18 2-deoxy-2-fluoro-D-glucose PET in the preoperative staging of breast cancer: Comparison with the standard staging procedures. Eur J Nucl Med. 2001;28:351–8. - PubMed
-
- Greco M, Crippa F, Agresti R, Seregni E, Gerali A, Giovanazzi R, et al. Axillary lymph node staging in breast cancer by 2-fluoro-2-deoxy-D-glucose-positron emission tomography: Clinical evaluation and alternative management. J Natl Cancer Inst. 2001;93:630–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical