

From re-emergence to hyperendemicity: the natural history of the dengue epidemic in Brazil
- PMID: 21245922
- PMCID: PMC3014978
- DOI: 10.1371/journal.pntd.0000935
From re-emergence to hyperendemicity: the natural history of the dengue epidemic in Brazil
Abstract
Background: dengue virus (DENV) was reintroduced into Brazil in 1986 and by 1995 it had spread throughout the country. In 2007 the number of dengue hemorrhagic fever (DHF) cases more than doubled and a shift in the age distribution was reported. While previously the majority of DHF cases occurred among adults, in 2007 53% of cases occurred in children under 15 years old. The reasons for this shift have not been determined.
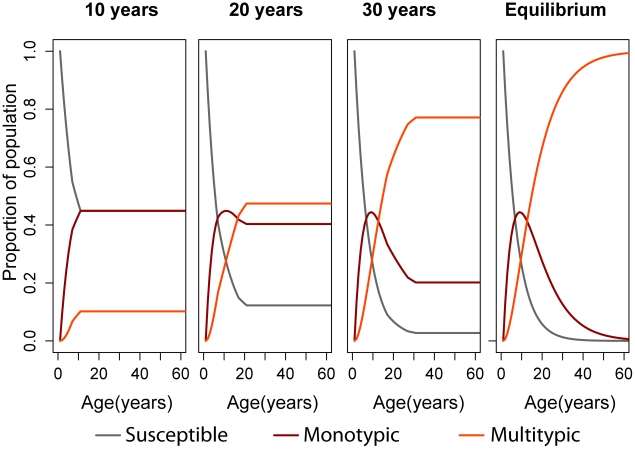
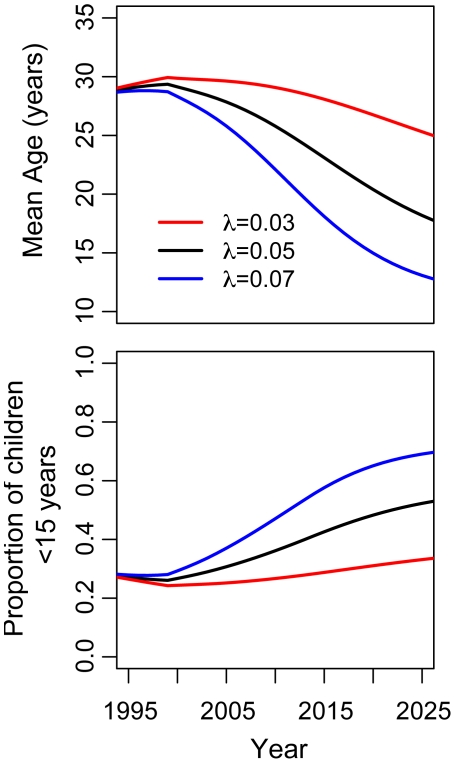
Methods and findings: age stratified cross-sectional seroepidemiologic survey conducted in Recife, Brazil in 2006. Serostatus was determined by ELISA based detection of Dengue IgG. We estimated time-constant and time-varying forces of infection of DENV between 1986 and 2006. We used discrete-time simulation to estimate the accumulation of monotypic and multitypic immunity over time in a population previously completely susceptible to DENV. We projected the age distribution of population immunity to dengue assuming similar hazards of infection in future years. The overall prevalence of DENV IgG was 0.80 (n = 1427). The time-constant force of infection for the period was estimated to be 0.052 (95% CI 0.041, 0.063), corresponding to 5.2% of susceptible individuals becoming infected each year by each serotype. Simulations show that as time since re-emergence of dengue goes by, multitypic immunity accumulates in adults while an increasing proportion of susceptible individuals and those with monotypic immunity are among young age groups. The median age of those monotypically immune can be expected to shift from 24 years, 10 years after introduction, to 13 years, 50 years after introduction. Of those monotypically immune, the proportion under 15 years old shifts from 27% to 58%. These results are consistent with the dengue notification records from the same region since 1995.
Interpretation: assuming that persons who have been monotypically exposed are at highest risk for severe dengue, the shift towards younger patient ages observed in Brazil can be partially explained by the accumulation of multitypic immunity against DENV-1, 2, and 3 in older age groups, 22 years after the re-introduction of these viruses. Serotype specific seroepidemiologic studies are necessary to accurately estimate the serotype specific forces of infection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


 (DENV 1, 2 and 3) = 0.05.
(DENV 1, 2 and 3) = 0.05.
References
-
- Gubler DJ. Cities spawn epidemic dengue viruses. Nat Med. 2004;10:129–130. - PubMed
-
- Kyle JL, Harris E. Global spread and persistence of dengue. Annu Rev Microbiol. 2008;62:71–92. - PubMed
-
- Halstead SB. Dengue in the Americas and Southeast Asia: do they differ? Rev Panam Salud Publica. 2006;20:407–415. - PubMed
-
- Halstead SB, Scanlon JE, Umpaivit P, Udomsakdi S. Dengue and chikungunya virus infection in man in Thailand, 1962-1964. IV. Epidemiologic studies in the Bangkok metropolitan area. Am J Trop Med Hyg. 1969;18:997–1021. - PubMed
-
- Balmaseda A, Hammond SN, Perez L, Tellez Y, Saborio SI, et al. Serotype-specific differences in clinical manifestations of dengue. Am J Trop Med Hyg. 2006;74:449–456. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
