

Deficits in the management of patients with adrenocortical carcinoma in Germany
- PMID: 21246024
- PMCID: PMC3021904
- DOI: 10.3238/arztebl.2010.0885
Deficits in the management of patients with adrenocortical carcinoma in Germany
Abstract
Background: Adrenocortical carcinoma (ACC) is a rare tumor with a poor prognosis. Often, the physicians who first treat patients with ACC have no prior experience with the disease. The aim of our study was to evaluate the quality of medical care for patients with ACC in Germany.
Methods: Data from the German ACC registry were analyzed with regard to the patients' preoperative diagnostic evaluation, histopathological reporting, and clinical follow-up. The findings were compared with the recommendations of the European Network for the Study of Adrenal Tumors (ENSAT).
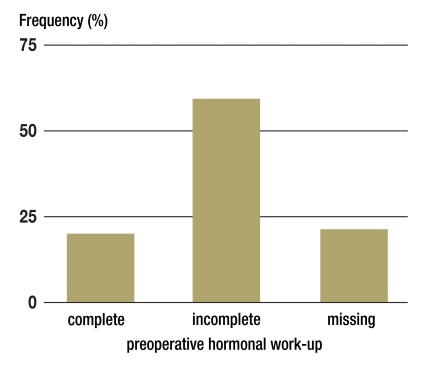
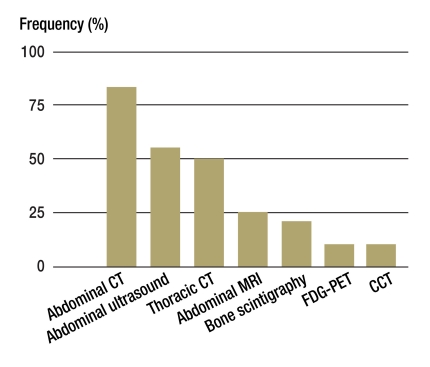
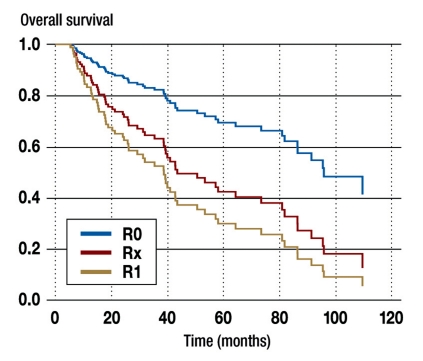
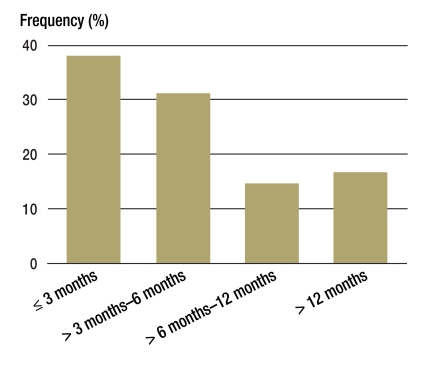
Results: Data were analyzed from 387 patients who had been given an initial diagnosis of ACC in the years 1998 to 2009. 21% of them underwent no hormonal evaluation before surgery, and 59% underwent an inadequate hormonal evaluation. This exposed the patients to unnecessary perioperative risks and impaired their follow-up. 48% did not undergo CT scanning of the chest, even though the lungs are the most frequent site of metastases of ACC. For 13% of the patients, the diagnosis of ACC was later revised by a reference pathologist. For 11% of the patients, the histopathology report contained no information about resection status, even though this is an important determinant of further treatment and prognosis. Optimal management requires re-staging at three-month intervals, yet some patients underwent re-staging only after a longer delay, or not at all.
Conclusion: We have identified significant deficits in the care of patients with ACC in Germany. We suspect that the situation is similar for other rare diseases. The prerequisite to better care is close and early cooperation of the treating physicians with specialized centers.
Figures
Comment in
-
Deficits in the management of patients with adrenocortical carcinoma in Germany. Statements cannot be substantiated.Dtsch Arztebl Int. 2011 May;108(19):339; author reply 339-40. doi: 10.3238/arztebl.2011.0339a. Epub 2011 May 13. Dtsch Arztebl Int. 2011. PMID: 21637638 Free PMC article. No abstract available.
References
-
- Fassnacht M, Allolio B. Clinical management of adrenocortical carcinoma. Best Pract Res Clin Endocrinol Metab. 2009;23:273–289. - PubMed
-
- Kebebew E, Reiff E, Duh QY, Clark OH, McMillan A. Extent of Disease at Presentation and Outcome for Adrenocortical Carcinoma: Have We Made Progress? World J Surg. 2006;30:872–878. - PubMed
-
- Bilimoria KY, Shen WT, Elaraj D, et al. Adrenocortical carcinoma in the United States: treatment utilization and prognostic factors. Cancer. 2008;113:3130–3136. - PubMed
-
- Abiven G, Coste J, Groussin L, et al. Clinical and biological features in the prognosis of adrenocortical cancer: poor outcome of cortisol-secreting tumors in a series of 202 consecutive patients. J Clin Endocrinol Metab. 2006;91:2650–2655. - PubMed
-
- Johanssen S, Fassnacht M, Brix D, et al. Das Nebennierenkarzinom - Diagnostik und Therapie. [Adrenocortical carcinoma: Diagnostic work-up and treatment] Urologe A. 2008;47:172–181. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical