

Modern triage in the emergency department
- PMID: 21246025
- PMCID: PMC3021905
- DOI: 10.3238/arztebl.2010.0892
Modern triage in the emergency department
Abstract
Background: Because the volume of patient admissions to an emergency department (ED) cannot be precisely planned, the available resources may become overwhelmed at times ("crowding"), with resulting risks for patient safety. The aim of this study is to identify modern triage instruments and assess their validity and reliability.
Methods: Review of selected literature retrieved by a search on the terms "emergency department" and "triage."
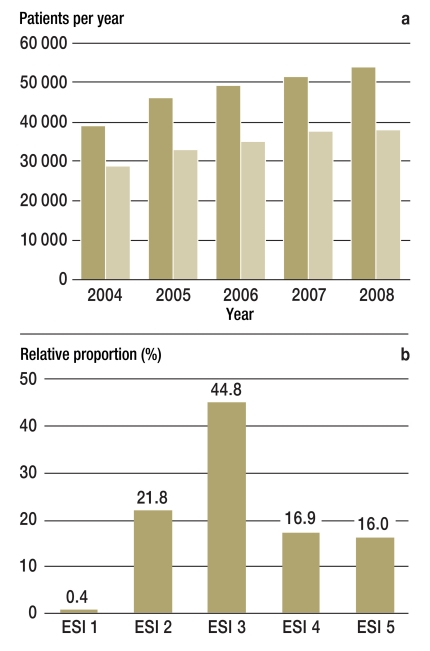
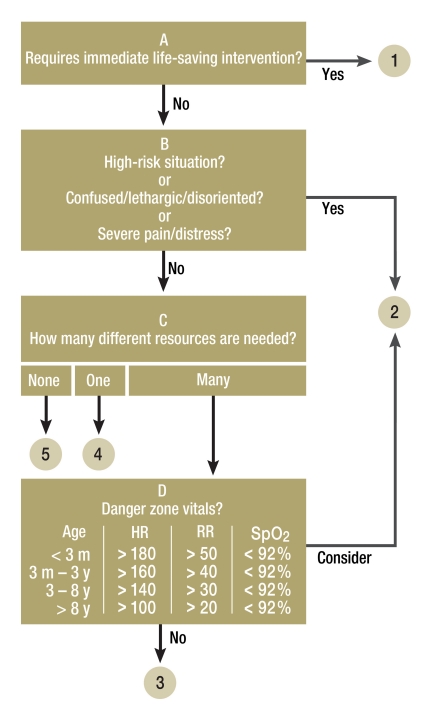
Results: Emergency departments around the world use different triage systems to assess the severity of incoming patients' conditions and assign treatment priorities. Our study identified four such instruments: the Australasian Triage Scale (ATS), the Canadian Triage and Acuity Scale (CTAS), the Manchester Triage System (MTS), and the Emergency Severity Index (ESI). Triage instruments with 5 levels are superior to those with 3 levels in both validity and reliability (p<0.01). Good to very good reliability has been shown for the best-studied instruments, CTAS and ESI (κ-statistics: 0.7 to 0.95), while ATS and MTS have been found to be only moderately reliable (κ-statistics: 0.3 to 0.6). MTS and ESI are both available in German; of these two, only the ESI has been validated in German-speaking countries.
Conclusion: Five-level triage systems are valid and reliable methods for assessment of the severity of incoming patients' conditions by nursing staff in the emergency department. They should be used in German emergency departments to assign treatment priorities in a structured and dependable fashion.
Figures
Comment in
-
Correspondence (letter to the editor): Easily done without triage models.Dtsch Arztebl Int. 2011 Apr;108(16):281-2; author reply 282-3. doi: 10.3238/arztebl.2011.0281b. Epub 2011 Apr 22. Dtsch Arztebl Int. 2011. PMID: 21603563 Free PMC article. No abstract available.
-
Correspondence (letter to the editor): Lack of resources.Dtsch Arztebl Int. 2011 Apr;108(16):281; author reply 282-3. doi: 10.3238/arztebl.2011.0281a. Epub 2011 Apr 22. Dtsch Arztebl Int. 2011. PMID: 21603564 Free PMC article. No abstract available.
-
Correspondence (letter to the editor): No system should be preferred.Dtsch Arztebl Int. 2011 Apr;108(16):282; author reply 282-3. doi: 10.3238/arztebl.2011.0282a. Epub 2011 Apr 22. Dtsch Arztebl Int. 2011. PMID: 21603566 Free PMC article. No abstract available.
References
-
- Pitts SR, Niska RW, Xu J, Burt CW. National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl Health Stat Report. 2008:1–38. - PubMed
-
- Steffen W, Tempka A, Klute G. Falsche Patientenanreize in der Ersten Hilfe der Krankenhäuser. Dtsch Arztebl. 2007;104:1088–1091.
-
- Schellein O, Ludwig-Pistor F, Bremerich DH. Manchester triage system: Process optimization in the interdisciplinary emergency department. Anaesthesist. 2008;58:163–170. - PubMed
-
- Rutschmann OT, Siber RS, Hugli OW. Empfehlung der Schweizerischen Gesellschaft für Notfall- und Rettungsmedizin (SGNOR) zur Triage in Schweizer Notfallstationen. Schweiz Ärztezeitung. 2009;90:1–2.
-
- Fernandes CM, Tanabe P, Gilboy N, et al. Five-level triage: a report from the ACEP/ENA Five-level Triage Task Force. J Emerg Nurs. 2005;31:39–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources