

Pilot clinical study for quantitative spectral diagnosis of non-melanoma skin cancer
- PMID: 21246575
- PMCID: PMC3059518
- DOI: 10.1002/lsm.21009
Pilot clinical study for quantitative spectral diagnosis of non-melanoma skin cancer
Abstract
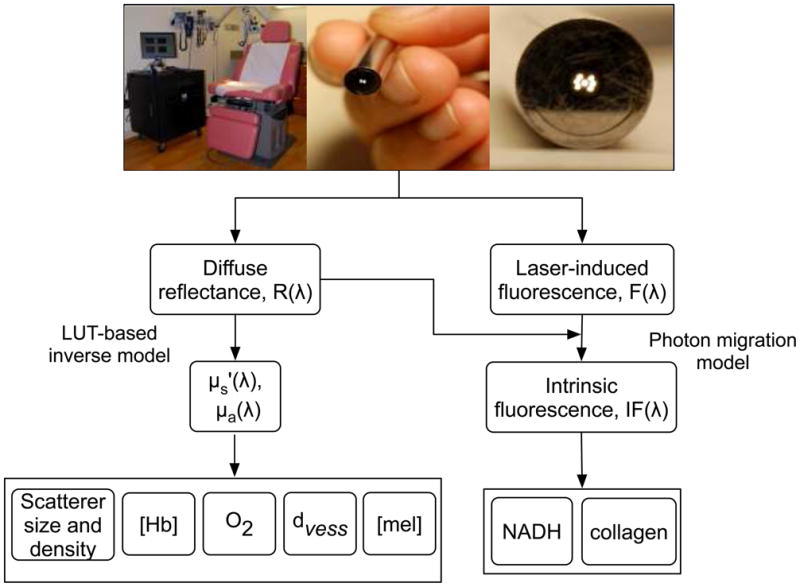
Background: Several research groups have demonstrated the non-invasive diagnostic potential of diffuse optical spectroscopy (DOS) and laser-induced fluorescence (LIF) techniques for early cancer detection. By combining both modalities, one can simultaneously measure quantitative parameters related to the morphology, function and biochemical composition of tissue and use them to diagnose malignancy. The objective of this study was to use a quantitative reflectance/fluorescence spectroscopic technique to determine the optical properties of normal skin and non-melanoma skin cancers and the ability to accurately classify them. An additional goal was to determine the ability of the technique to differentiate non-melanoma skin cancers from normal skin.
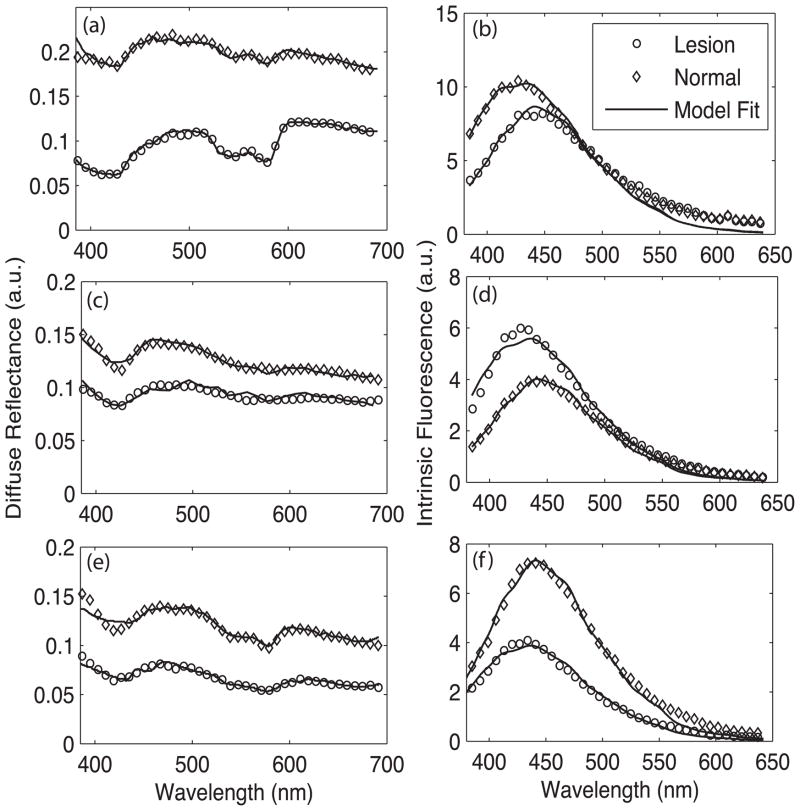
Study design: The study comprised 48 lesions measured from 40 patients scheduled for a biopsy of suspected non-melanoma skin cancers. White light reflectance and laser-induced fluorescence spectra (wavelength range = 350-700 nm) were collected from each suspected lesion and adjacent clinically normal skin using a custom-built, optical fiber-based clinical instrument. After measurement, the skin sites were biopsied and categorized according to histopathology. Using a quantitative model, we extracted various optical parameters from the measured spectra that could be correlated to the physiological state of tissue.
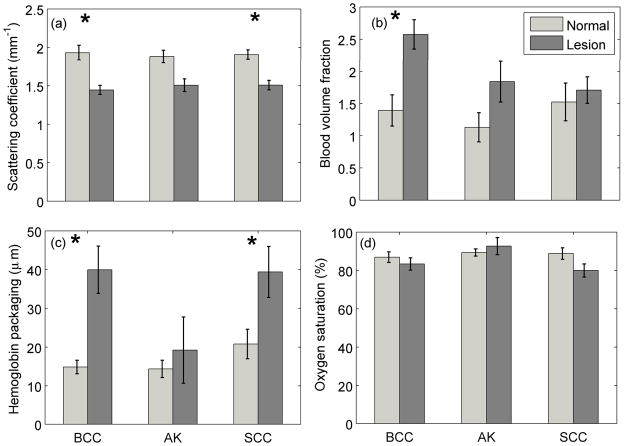
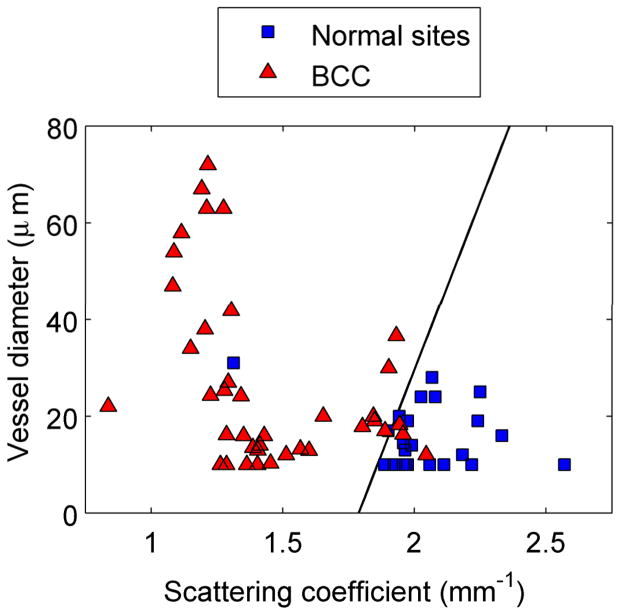
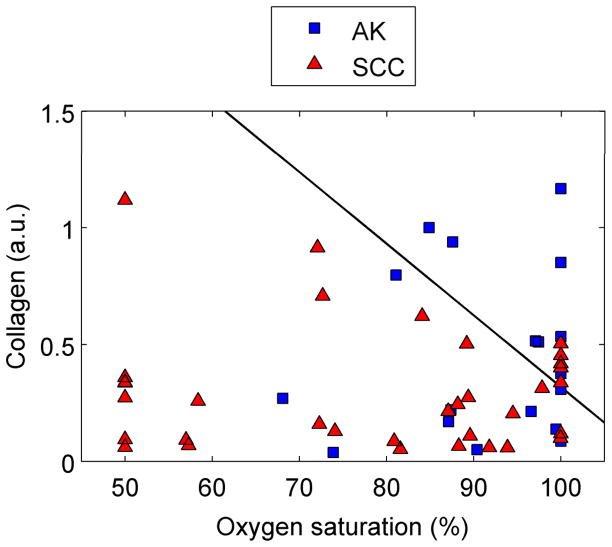
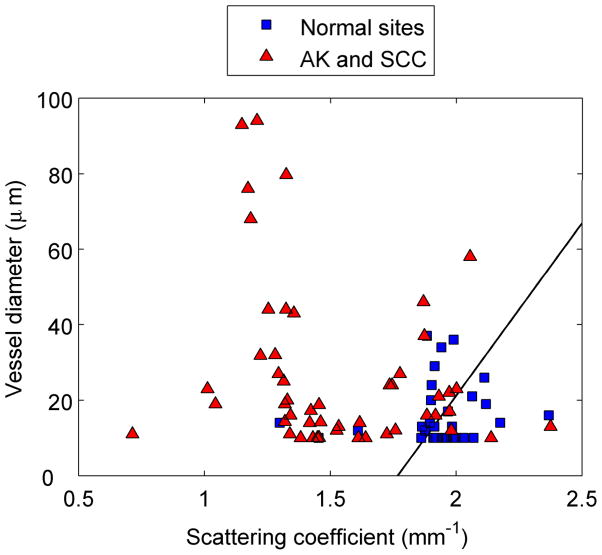
Results: Scattering from cancerous lesions was significantly lower than normal skin for every lesion group, whereas absorption parameters were significantly higher. Using numerical cut-offs for our optical parameters, our clinical instrument could classify basal cell carcinomas with a sensitivity and specificity of 94% and 89%, respectively. Similarly, the instrument classified actinic keratoses and squamous cell carcinomas with a sensitivity of 100% and specificity of 50%.
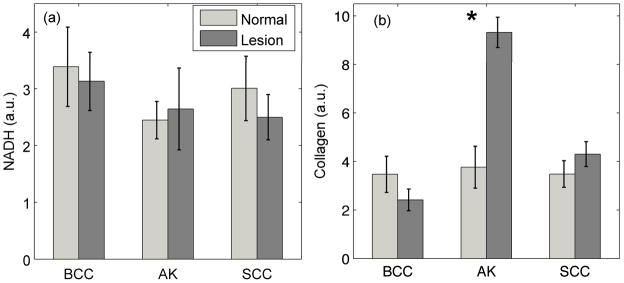
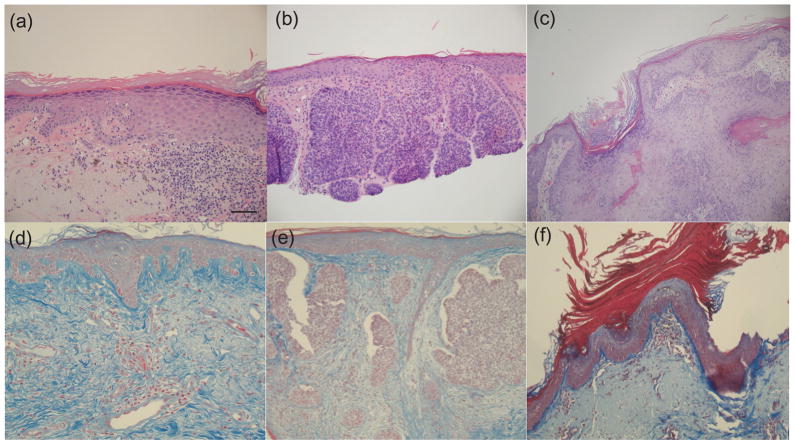
Conclusion: The measured optical properties and fluorophore contributions of normal skin and non-melanoma skin cancers are significantly different from each other and correlate well with tissue pathology. A diagnostic algorithm that combines these extracted properties holds promise for the potential non-invasive diagnosis of skin cancer.
Copyright © 2010 Wiley-Liss, Inc.
Conflict of interest statement
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics. CA: A Cancer Journal for Clinicians; 2010. - PubMed
-
- Moreno G, Tran H, Chia A, Lim A, Shumack S. Prospective study to assess general practitioners' dermatological diagnostic skills in a referral setting. Australasian Journal of Dermatology. 2007;48(2):77. - PubMed
-
- Kittler H, Pehamberger H, Wolff K, Binder M. Diagnostic accuracy of dermoscopy. Lancet Oncol. 2002;3(3):159–165. - PubMed
-
- Marchesini R, Cascinelli N, Brambilla M, Clemente C, Mascheroni L, Pignoli E, Testori A, Venturoli D. In vivo spectrophotometric evaluation of neoplastic and non-neoplastic skin pigmented lesions. II: Discriminant analysis between nevus and melanoma. Photochem Photobiol. 1992;55(4):515–522. - PubMed
-
- Wallace VP, Crawford DC, Mortimer PS, Ott RJ, Bamber JC. Spectrophotometric assessment of pigmented skin lesions: methods and feature selection for evaluation of diagnostic performance. Phys Med Biol. 2000;45(3):735–751. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
