

Effect of occult metastases on survival in node-negative breast cancer
- PMID: 21247310
- PMCID: PMC3044504
- DOI: 10.1056/NEJMoa1008108
Effect of occult metastases on survival in node-negative breast cancer
Abstract
Background: Retrospective and observational analyses suggest that occult lymph-node metastases are an important prognostic factor for disease recurrence or survival among patients with breast cancer. Prospective data on clinical outcomes from randomized trials according to sentinel-node involvement have been lacking.
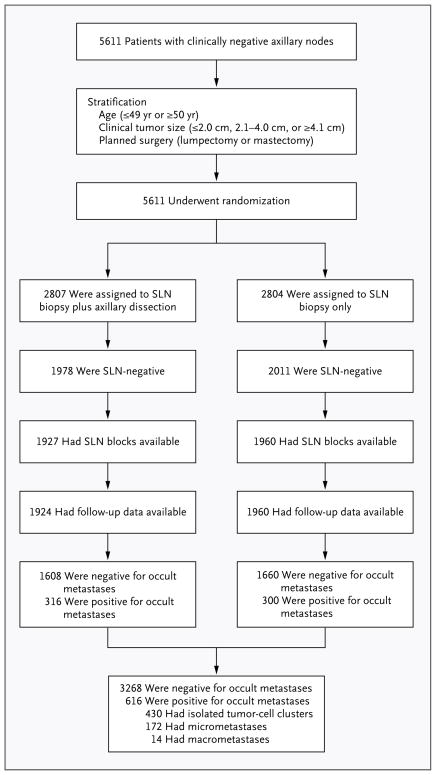
Methods: We randomly assigned women with breast cancer to sentinel-lymph-node biopsy plus axillary dissection or sentinel-lymph-node biopsy alone. Paraffin-embedded tissue blocks of sentinel lymph nodes obtained from patients with pathologically negative sentinel lymph nodes were centrally evaluated for occult metastases deeper in the blocks. Both routine staining and immunohistochemical staining for cytokeratin were used at two widely spaced additional tissue levels. Treating physicians were unaware of the findings, which were not used for clinical treatment decisions. The initial evaluation at participating sites was designed to detect all macrometastases larger than 2 mm in the greatest dimension.
Results: Occult metastases were detected in 15.9% (95% confidence interval [CI], 14.7 to 17.1) of 3887 patients. Log-rank tests indicated a significant difference between patients in whom occult metastases were detected and those in whom no occult metastases were detected with respect to overall survival (P=0.03), disease-free survival (P=0.02), and distant-disease-free interval (P=0.04). The corresponding adjusted hazard ratios for death, any outcome event, and distant disease were 1.40 (95% CI, 1.05 to 1.86), 1.31 (95% CI, 1.07 to 1.60), and 1.30 (95% CI, 1.02 to 1.66), respectively. Five-year Kaplan-Meier estimates of overall survival among patients in whom occult metastases were detected and those without detectable metastases were 94.6% and 95.8%, respectively.
Conclusions: Occult metastases were an independent prognostic variable in patients with sentinel nodes that were negative on initial examination; however, the magnitude of the difference in outcome at 5 years was small (1.2 percentage points). These data do not indicate a clinical benefit of additional evaluation, including immunohistochemical analysis, of initially negative sentinel nodes in patients with breast cancer. (Funded by the National Cancer Institute; ClinicalTrials.gov number, NCT00003830.).
Figures

References
-
- Saphir O, Amromin GD. Obscure axillary lymph node metastases in carcinoma of the breast. Cancer. 1948;1:238–41. - PubMed
-
- Dowlatshahi K, Fan M, Snider HC, Habib FA. Lymph node micrometastases from breast carcinoma: reviewing the dilemma. Cancer. 1997;80:1188–97. - PubMed
-
- de Boer M, van Dijck JA, Bult P, Borm GF, Tjan-Heijnen VC. Breast cancer prognosis and occult lymph node metastases, isolated tumor cells, and micrometastases. J Natl Cancer Inst. 2010;102:410–25. - PubMed
-
- Weaver DL. Sentinel lymph nodes and breast carcinoma: which micrometastases are clinically significant? Am J Surg Pathol. 2003;27:842–5. - PubMed
-
- Krag DN, Anderson SJ, Julian TB, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase III trial. Lancet Oncol. 2007;8:881–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical