

What should we include in a cultural competence curriculum? An emerging formative evaluation process to foster curriculum development
- PMID: 21248602
- PMCID: PMC3046368
- DOI: 10.1097/ACM.0b013e3182087314
What should we include in a cultural competence curriculum? An emerging formative evaluation process to foster curriculum development
Abstract
Purpose: To identify, prioritize, and organize components of a cultural competence curriculum to address disparities in cardiovascular disease.
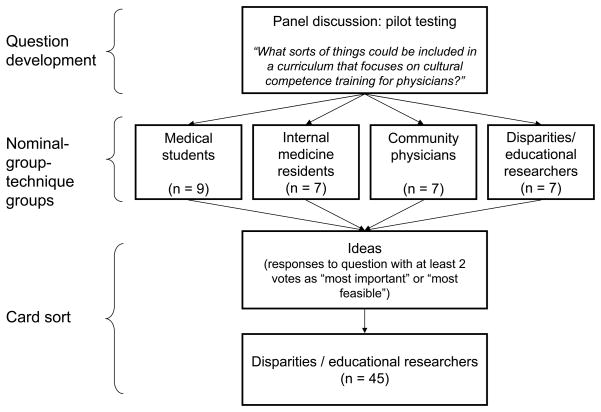
Method: In 2006, four separate nominal group technique sessions were conducted with medical students, residents, community physicians, and academic physicians to generate and prioritize a list of concepts (i.e., ideas) to include in a curriculum. Afterward, 45 educators and researchers organized and prioritized the concepts using a card-sorting exercise. Multidimensional scaling (MDS) and hierarchical cluster analysis produced homogeneous groupings of related concepts and generated a cognitive map. The main outcome measures were the number of cultural competence concepts, their relative ranks, and the cognitive map.
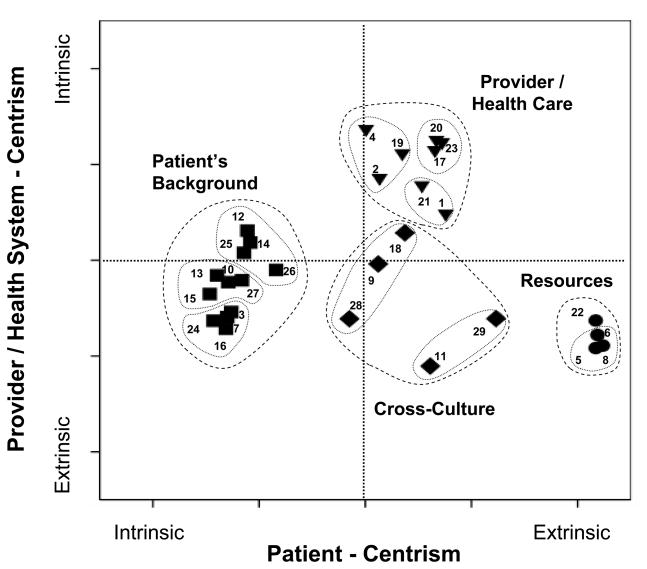
Results: Thirty participants generated 61 concepts; 29 were identified by at least two participants. The cognitive map organized concepts into four clusters, interpreted as (1) patient's cultural background (e.g., information on cultures, habits, values), (2) provider and health care (e.g., clinical skills, awareness of one's bias, patient centeredness, professionalism), communication skills (e.g., history, stereotype avoidance, health disparities epidemiology), (3) cross-culture (e.g., idiomatic expressions, examples of effective communication), and (4) resources to manage cultural diversity (e.g., translator guides, instructions, community resources). The MDS two-dimensional solution demonstrated a good fit (stress = 0.07; R² = 0.97).
Conclusions: A novel, combined approach allowed stakeholders' inputs to identify and cognitively organize critical domains used to guide development of a cultural competence curriculum. Educators may use this approach to develop and organize educational content for their target audiences, especially in ill-defined areas like cultural competence.
Figures
References
-
- Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Institute of Medicine, National Academy of Sciences; Washington, D.C: 2002.
-
- Lie D, Boker J, Cleveland E. Using the tool for assessing cultural competence training (TACCT) to measure faculty and medical student perceptions of cultural competence instruction in the first three years of the curriculum. Acad Med. 2006. [Accessed November 19, 2010]. pp. 557–564 . http://journals.lww.com/academicmedicine/Fulltext/2006/06000/Using_the_T.... - PubMed
-
- Betancourt JR, Green AR. Commentary: linking cultural competence training to improved health outcomes: perspectives from the field. Acad Med. 2010. [Accessed November 19, 2010]. pp. 583–585. http://journals.lww.com/academicmedicine/Fulltext/2010/04000/Commentary_.... - PubMed
-
- Smith WR, Betancourt JR, Wynia MK, et al. Recommendations for teaching about racial and ethnic disparities in health and health care. Ann Intern Med. 2007;147(9):654–665. - PubMed
-
- Betancourt JR. Cross-cultural Medical Education: Conceptual Approaches and Frameworks for Evaluation. Acad Med. 2003. [Accessed November 19, 2010]. pp. 560–569. http://journals.lww.com/academicmedicine/Fulltext/2003/06000/Cross_cultu.... - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
