

EGC diagnosis of paroxysmal supraventricular tachycardias in patients without preexcitation
- PMID: 21251139
- PMCID: PMC6932539
- DOI: 10.1111/j.1542-474X.2010.00399.x
EGC diagnosis of paroxysmal supraventricular tachycardias in patients without preexcitation
Abstract
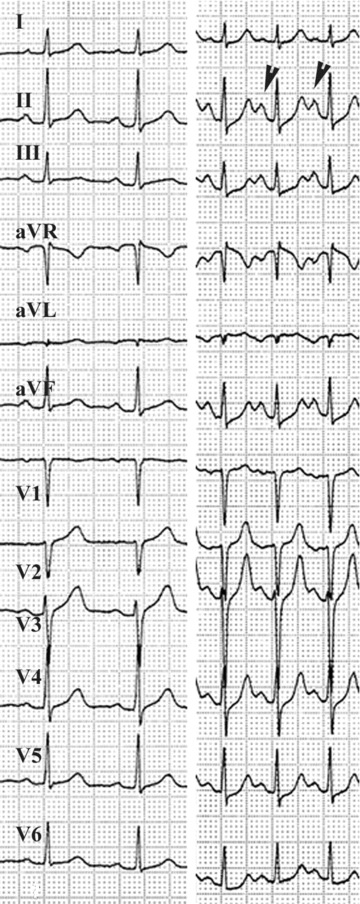
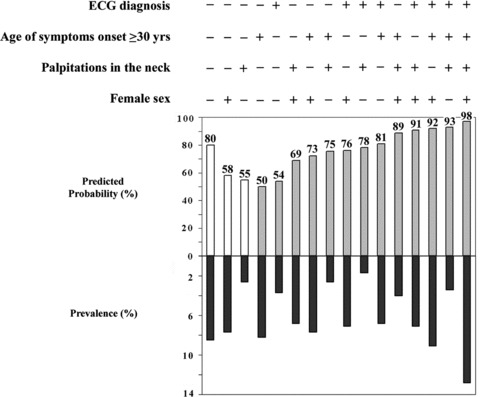
This review is aimed at discussing the diagnostic value of the different electrocardiographic criteria so far described in the differential diagnosis of the major forms of paroxysmal supraventricular tachycardias (PSVTs). The predictive value of different combinations of these independent electrocardiographic (ECG) signs in distinguishing atrioventricular reentrant tachycardias (AVRTs) through a concealed accessory pathway (AP) versus atrioventricular nodal reentrant tachycardias (AVNRTs) are discussed in detail. In addition, the adjunctive diagnostic value of simple, bedside clinical variables and their combinations to the ECG interpretation in differentiating both tachycardia mechanisms is also reviewed.
©2011, Wiley Periodicals, Inc.
Figures









References
-
- Porter MJ, Morton JB, Denman R, et al Influence of age and gender on the mechanism of supraventricular tachycardia. Heart Rhythm 2004;1:397–398. - PubMed
-
- Kalbfleisch SJ, El‐Atassi R, Calkins H, et al Differentiation of paroxysmal narrow QRS complex tachycardias using the 12‐lead electrocardiogram. J Am Coll Cardiol 1993;21:85–89. - PubMed
-
- Riva SI, Della Bella P, Fassini G, et al Value of analysis of ST segment changes during tachycardia in determining type of narrow QRS complex tachycardias. J Am Coll Cardiol 1996;27:1480–1485. - PubMed
-
- González‐Torrecilla E, Almendral J, Arenal A, et al Independent predictive accuracy of classical electrocardiographic criteria in the diagnosis of paroxysmal atrioventricular reciprocating tachycardias in patients without pre‐excitation. Europace 2008;10:624–628. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
