

Predicting functional decline in behavioural variant frontotemporal dementia
- PMID: 21252111
- PMCID: PMC3030765
- DOI: 10.1093/brain/awq348
Predicting functional decline in behavioural variant frontotemporal dementia
Abstract
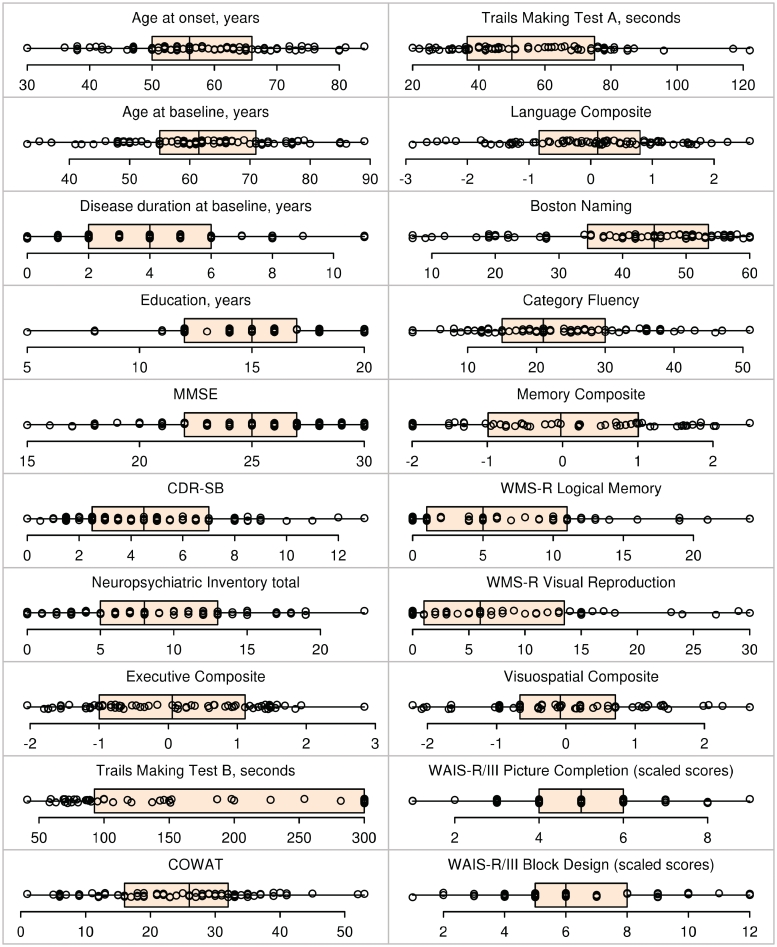
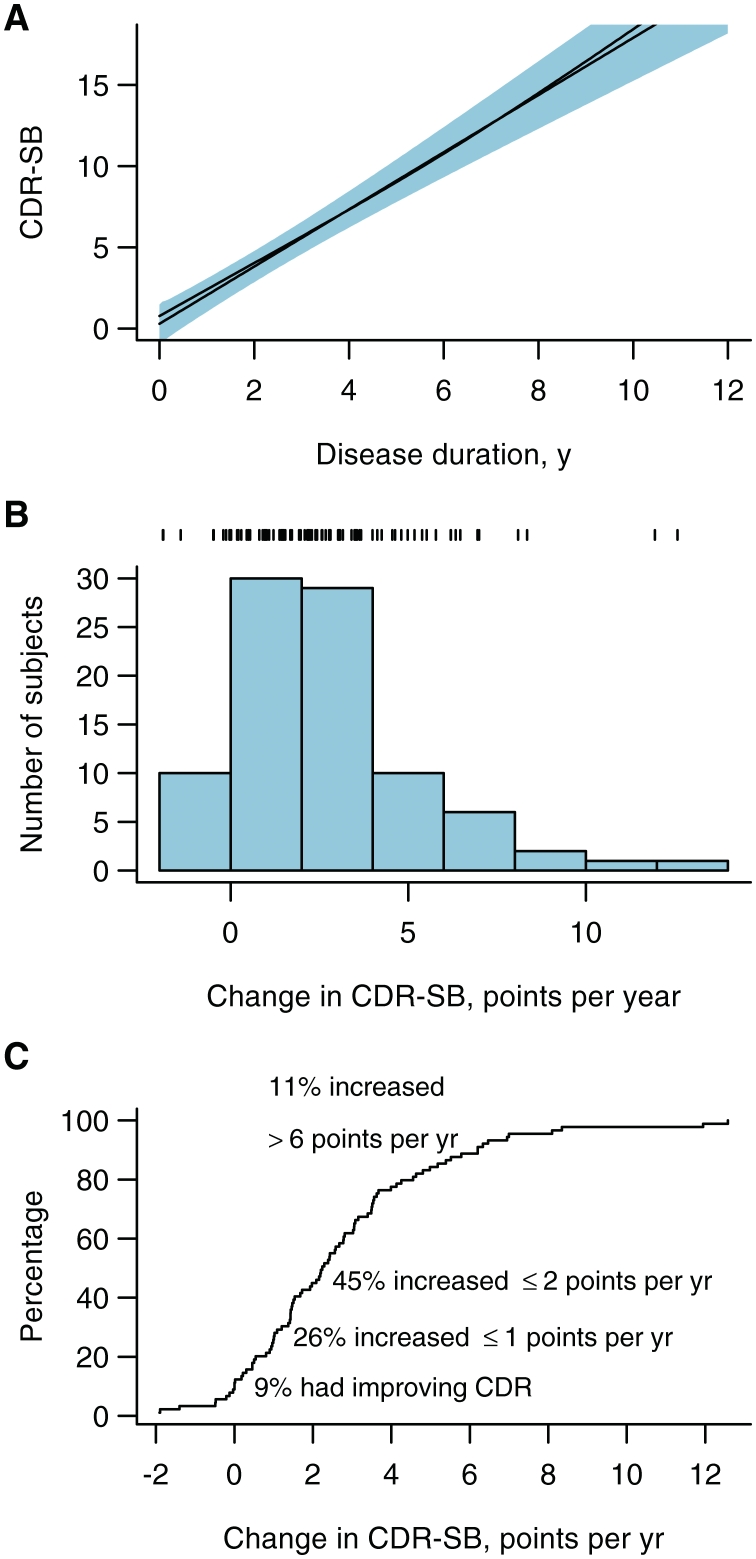
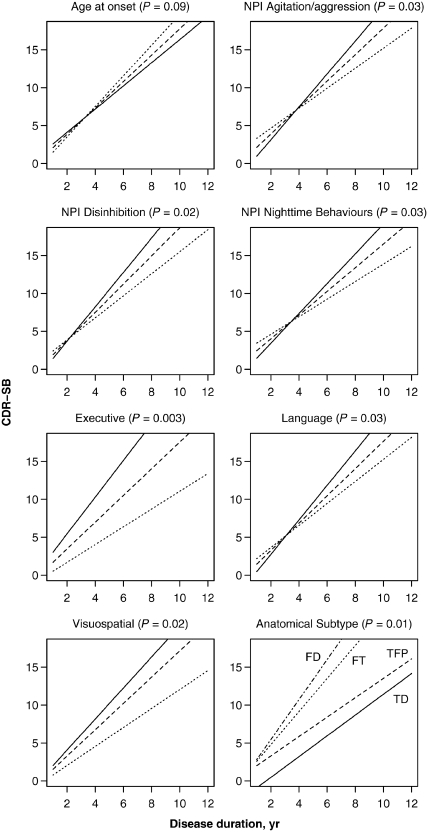
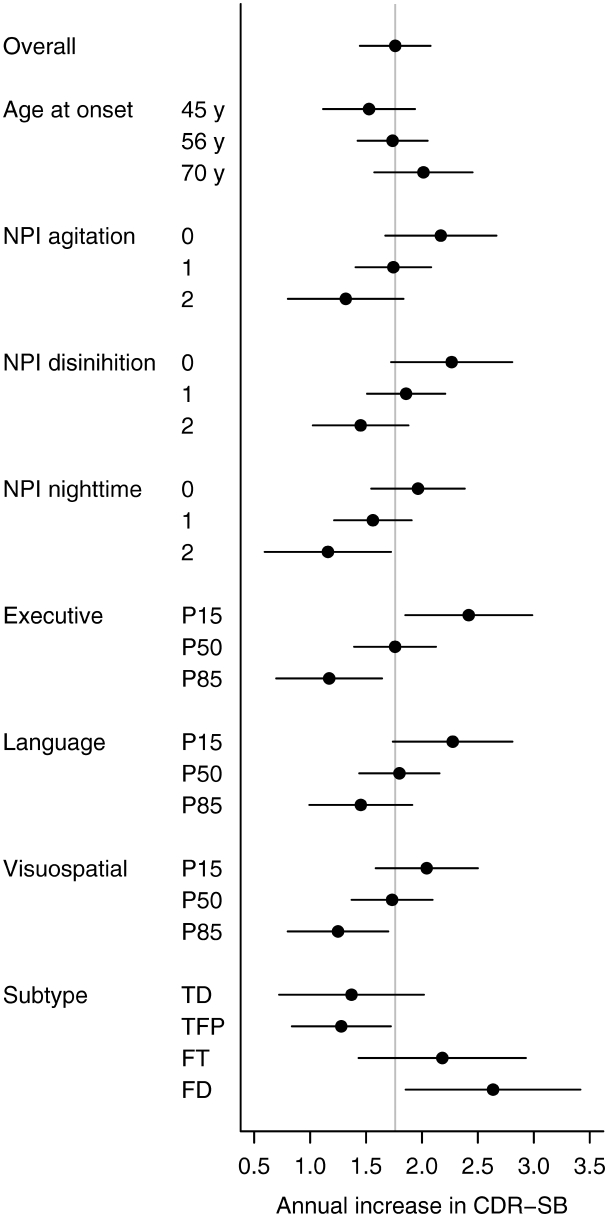
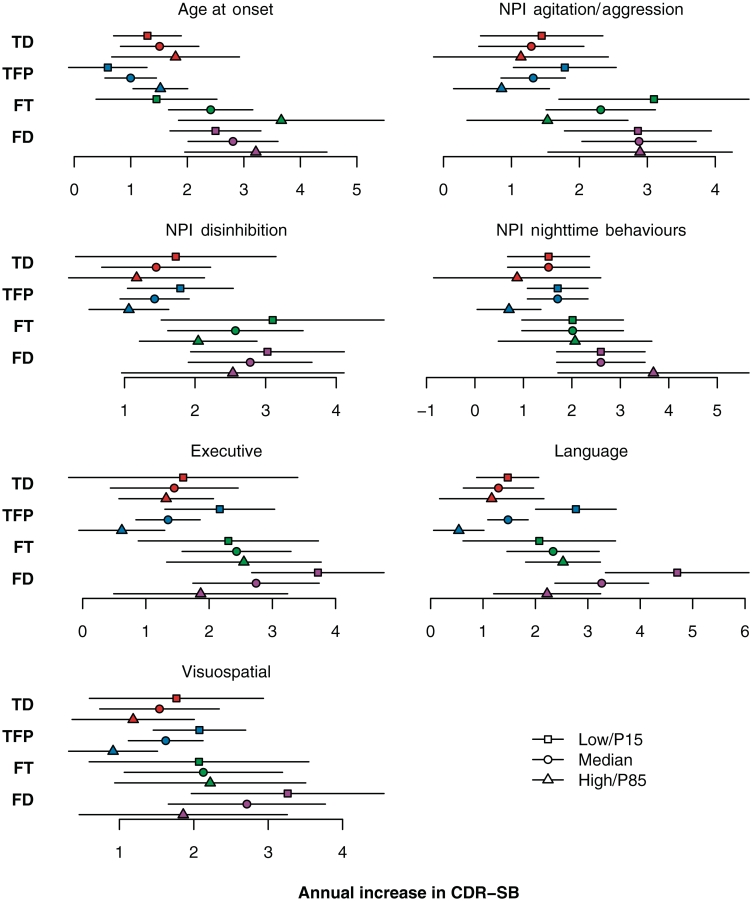
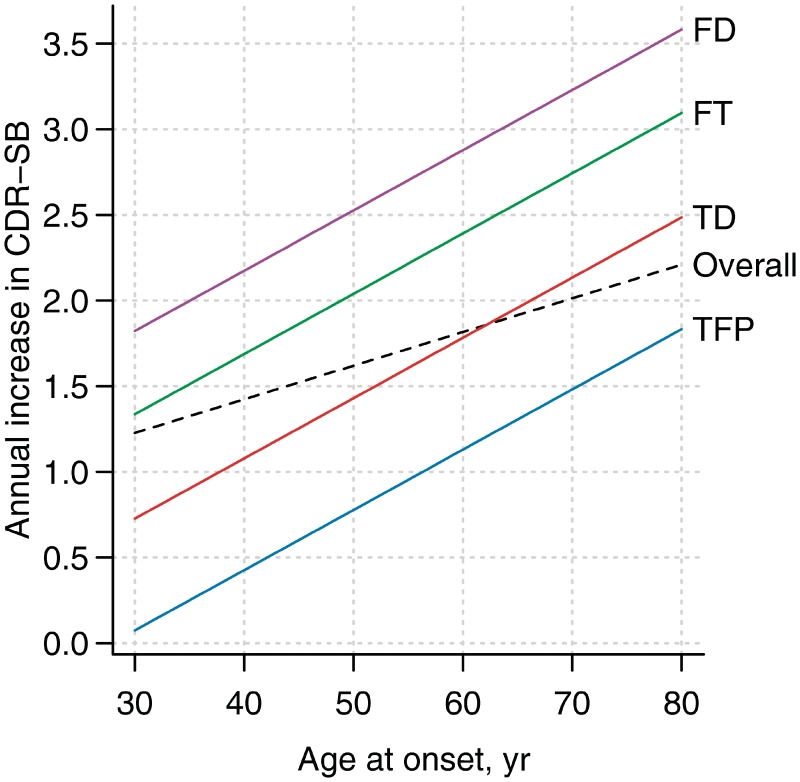
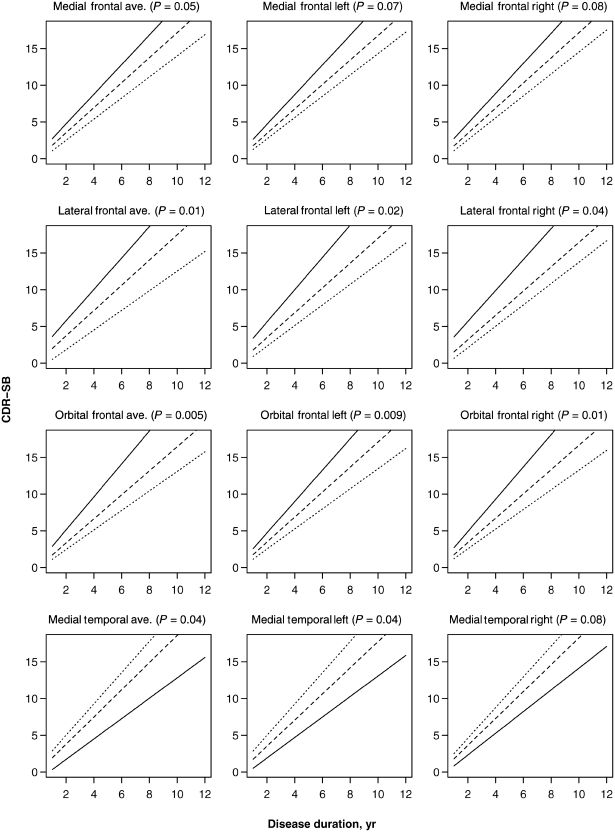
Behavioural variant frontotemporal dementia is characterized by a change in comportment. It is associated with considerable functional decline over the course of the illness albeit with sometimes dramatic variability among patients. It is unknown whether any baseline features, or combination of features, could predict rate of functional decline in behavioural variant frontotemporal dementia. The aim of this study was to investigate the effects of different baseline clinical, neuropsychological, neuropsychiatric, genetic and anatomic predictors on the rate of functional decline as measured by the Clinical Dementia Rating Sum of Boxes scale. We identified 86 subjects with behavioural variant frontotemporal dementia that had multiple serial Clinical Dementia Rating Sum of Boxes assessments (mean 4, range 2-18). Atlas-based parcellation was used to generate volumes for specific regions of interest at baseline. Volumes were utilized to classify subjects into different anatomical subtypes using the advanced statistical technique of cluster analysis and were assessed as predictor variables. Composite scores were generated for the neuropsychological domains of executive, language, memory and visuospatial function. Behaviours from the brief questionnaire form of the Neuropsychiatric Inventory were assessed. Linear mixed-effects regression modelling was used to determine which baseline features predict rate of future functional decline. Rates of functional decline differed across the anatomical subtypes of behavioural variant frontotemporal dementia, with faster rates observed in the frontal dominant and frontotemporal subtypes. In addition, subjects with poorer performance on neuropsychological tests of executive, language and visuospatial function, less disinhibition, agitation/aggression and night-time behaviours at presentation, and smaller medial, lateral and orbital frontal lobe volumes showed faster rates of decline. In many instances, the effect of the predictor variables observed across all subjects was also preserved within anatomical subtypes. Furthermore, some of the predictor variables improved our prediction of rate of functional decline after anatomical subtype was taken into account. In particular, age at onset was a highly significant predictor but only after adjusting for subtype. We also found that although some predictor variables, for example gender, Mini-Mental State Examination score, and apathy/indifference, did not affect the rate of functional decline; these variables were associated with the actual Clinical Dementia Rating Sum of Boxes score estimated for any given time-point. These findings suggest that in behavioural variant frontotemporal dementia, rate of functional decline is driven by the combination of anatomical pattern of atrophy, age at onset, and neuropsychiatric characteristics of the subject at baseline.
Figures
References
-
- Ashburner J, Friston KJ. Unified segmentation. Neuroimage. 2005;26:839–51. - PubMed
-
- Benton AL, Hamsher K. Manual. Iowa City: University of Iowa; 1989. Multilingual Aphasia Examination.
-
- Burke WJ, Miller JP, Rubin EH, Morris JC, Coben LA, Duchek J, et al. Reliability of the Washington University Clinical Dementia Rating. Arch Neurol. 1988;45:31–2. - PubMed
-
- Chiu WZ, Kaat LD, Seelaar H, Rosso SM, Boon AJ, Kamphorst W, et al. Survival in progressive supranuclear palsy and frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2010;81:441–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
