

Endothelial cell-specific deficiency of Ang II type 1a receptors attenuates Ang II-induced ascending aortic aneurysms in LDL receptor-/- mice
- PMID: 21252156
- PMCID: PMC3076204
- DOI: 10.1161/CIRCRESAHA.110.222844
Endothelial cell-specific deficiency of Ang II type 1a receptors attenuates Ang II-induced ascending aortic aneurysms in LDL receptor-/- mice
Abstract
Rationale: Human studies and mouse models have provided evidence for angiotensin II (Ang II)-based mechanisms as an underlying cause of aneurysms localized to the ascending aorta. In agreement with this associative evidence, we have published recently that Ang II infusion induces aneurysmal pathology in the ascending aorta.
Objective: The aim of this study was to define the role of angiotensin II type 1a (AT(1a)) receptors and their cellular location in Ang II-induced ascending aortic aneurysms (AAs).
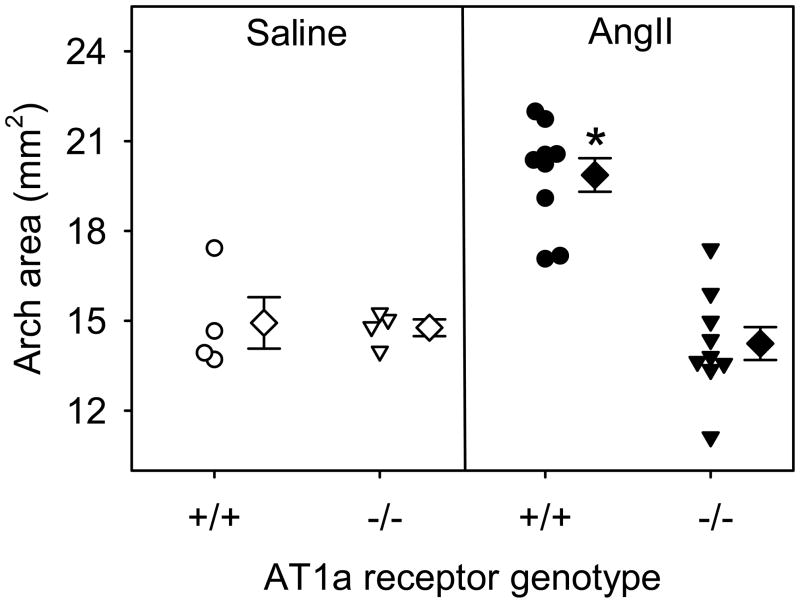
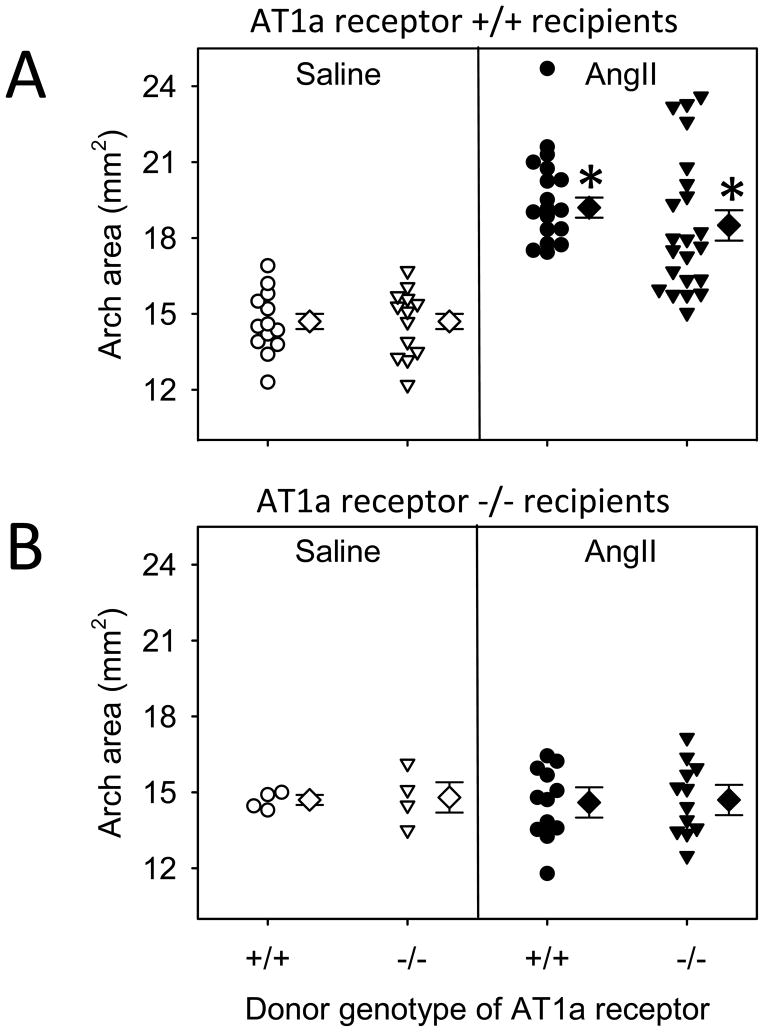
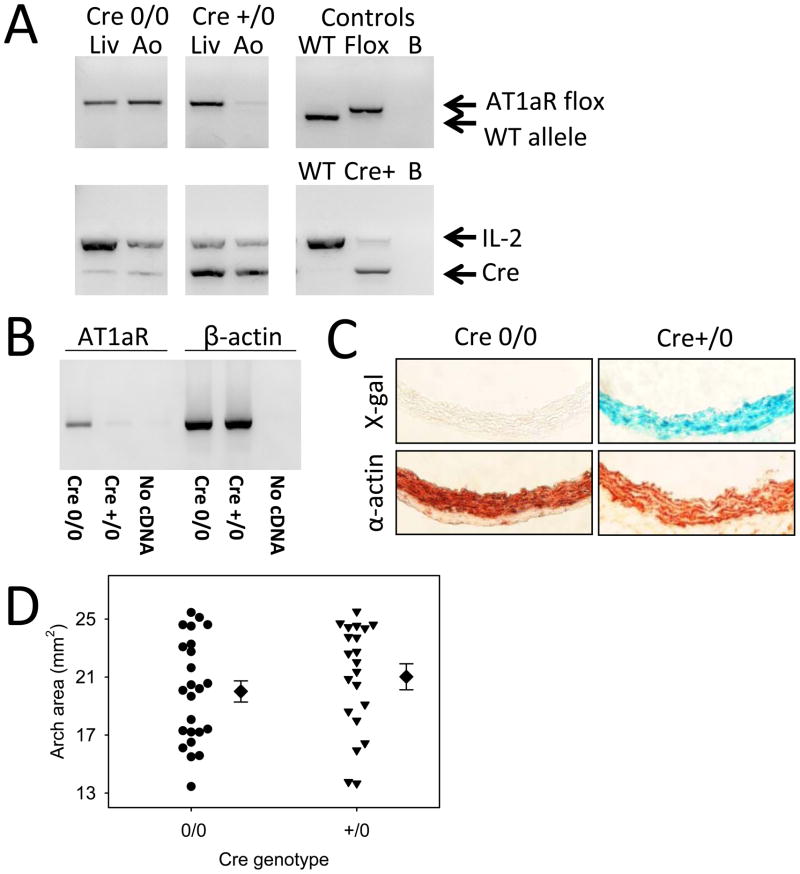
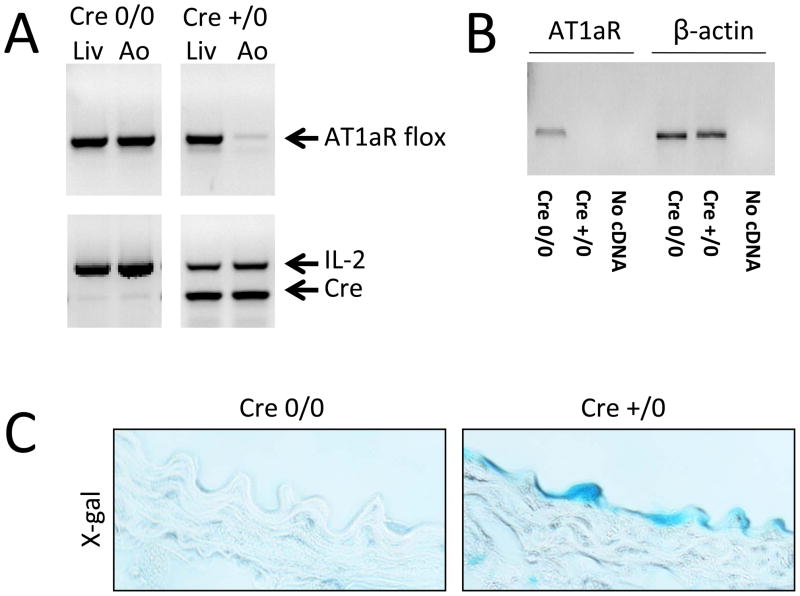
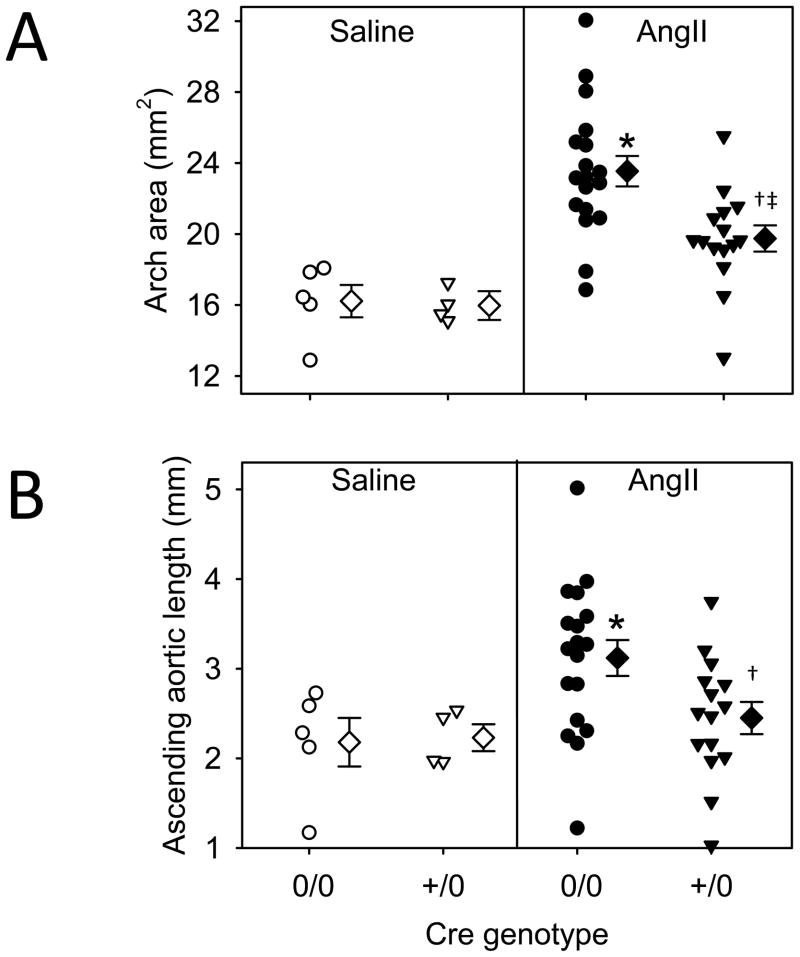
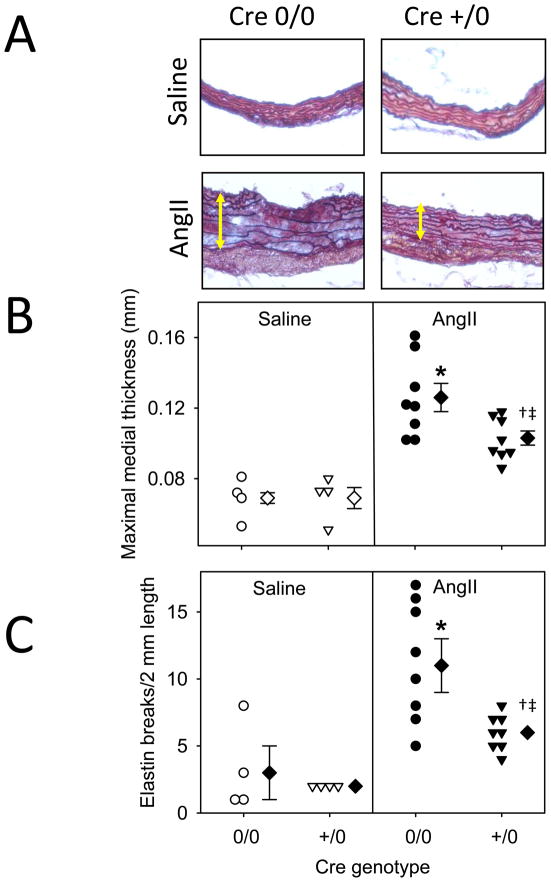
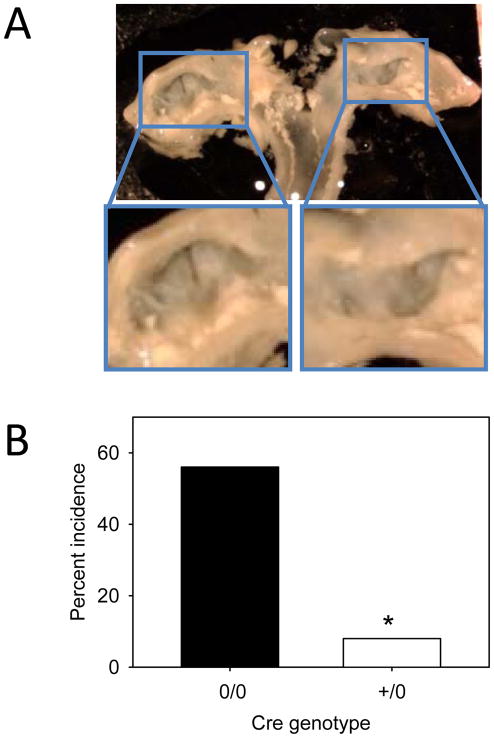
Methods and results: Male LDL receptor(-/-) mice were fed a saturated fat-enriched diet for 1 week before osmotic mini-pump implantation and infused with either saline or Ang II (1000 ng/kg per minute) for 28 days. Intimal surface areas of ascending aortas were measured to quantify ascending AAs. Whole body AT(1a) receptor deficiency ablated Ang II-induced ascending AAs (P<0.001). To determine the role of AT(1a) receptors on leukocytes, LDL receptor(-/-)×AT(1a) receptor(+/+) or AT(1a) receptor(-/-) mice were irradiated and repopulated with bone marrow-derived cells isolated from either AT(1a) receptor(+/+) or AT(1a) receptor(-/-) mice. Deficiency of AT(1a) receptors in bone marrow-derived cells had no effect on Ang II-induced ascending AAs. To determine the role of AT(1a) receptors on vascular wall cells, we developed AT(1a) receptor floxed mice with depletion on either smooth muscle or endothelial cells using Cre driven by either SM22 or Tek, respectively. AT(1a) receptor deletion in smooth muscle cells had no effect on ascending AAs. In contrast, endothelial-specific depletion attenuated this pathology.
Conclusions: Ang II infusion promotes aneurysms in the ascending aorta via stimulation of AT(1a) receptors that are expressed on endothelial cells.
Figures
Comment in
-
Parsing aortic aneurysms: more surprises.Circ Res. 2011 Mar 4;108(5):528-30. doi: 10.1161/CIRCRESAHA.111.240861. Circ Res. 2011. PMID: 21372288 Free PMC article.
References
-
- Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, Casey DE, Jr, Eagle KA, Hermann LK, Isselbacher EM, Kazerooni EA, Kouchoukos NT, Lytle BW, Milewicz DM, Reich DL, Sen S, Shinn JA, Svensson LG, Williams DM. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121:e266–369. - PubMed
-
- Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinically pertinent controversies and uncertainties. J Am Coll Cardiol. 2010;55:841–857. - PubMed
-
- Pannu H, Tran-Fadulu V, Papke CL, Scherer S, Liu Y, Presley C, Guo D, Estrera AL, Safi HJ, Brasier AR, Vick GW, Marian AJ, Raman CS, Buja LM, Milewicz DM. MYH11 mutations result in a distinct vascular pathology driven by insulin-like growth factor 1 and angiotensin II. Hum Mol Genet. 2007;16:3453–3462. - PMC - PubMed
-
- Habashi JP, Judge DP, Holm TM, Cohn RD, Loeys BL, Cooper TK, Myers L, Klein EC, Liu G, Calvi C, Podowski M, Neptune ER, Halushka MK, Bedja D, Gabrielson K, Rifkin DB, Carta L, Ramirez F, Huso DL, Dietz HC. Losartan, an AT1 antagonist, prevents aortic aneurysm in a mouse model of Marfan syndrome. Science. 2006;312:117–121. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
