

Review
doi: 10.1097/AOG.0b013e31820780e3.
Uterine leiomyomas: individualizing the approach to a heterogeneous condition
Affiliations
- PMID: 21252757
- PMCID: PMC3150866
- DOI: 10.1097/AOG.0b013e31820780e3
Item in Clipboard
Review
Uterine leiomyomas: individualizing the approach to a heterogeneous condition
Obstet Gynecol.
2011 Feb.
No abstract available
Figures
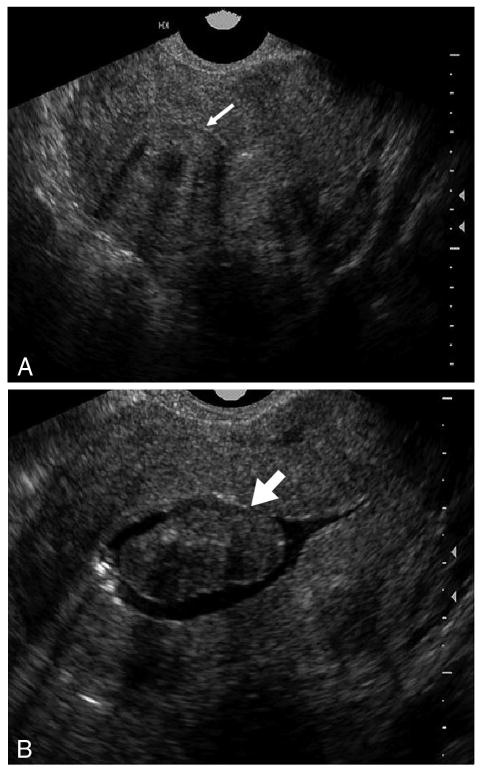
Class 0 submucosal leiomyoma. On transvaginal ultrasonography (A), a central myoma is seen, but the relationship to the endometrial cavity is unclear (thin arrow). With a sonohysterogram (B), the complete intracavitary extent is clarified (thick arrow).
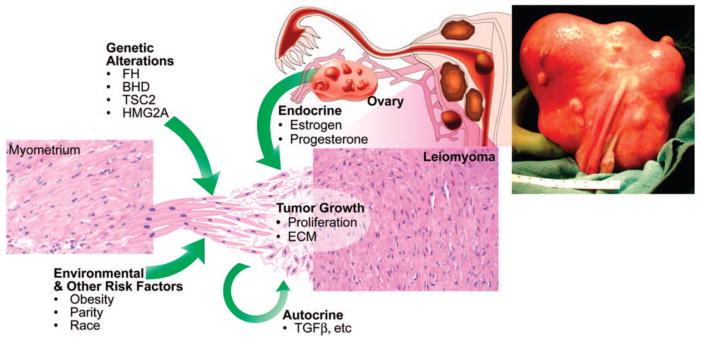
Etiology of uterine leiomyomas. Leiomyomas are heterogenous in their natural history and etiology. Hereditary defects in the FH, BHD, and TSC2 genes and somatic alterations affecting HMG2A genes contribute to the development of leiomyomas, as do risk factors such as obesity, parity, and race. Tumor growth occurs by an increase in tumor cell number and extracellular matrix production and is promoted by both endocrine and autocrine growth factors. Reprinted from Walker CL, Stewart EA. Uterine fibroids: the elephant in the room. Science 2005;308:1589–92. Reprinted with permission from the American Association for the Advancement of Science.
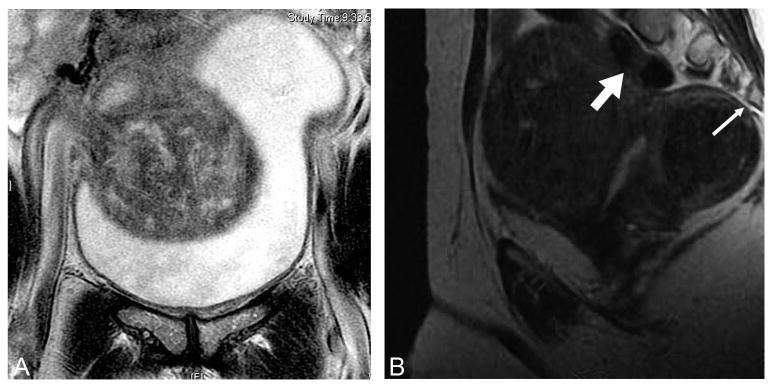
Magnetic resonance imaging (MRI) demonstrating leiomyoma compressing (A) the bladder and (B) the spine (thin arrow) and colon (thick arrow). Bulk symptoms from leiomyomas include decreased bladder capacity and outflow obstruction, constipation, back pain, and sciatica.
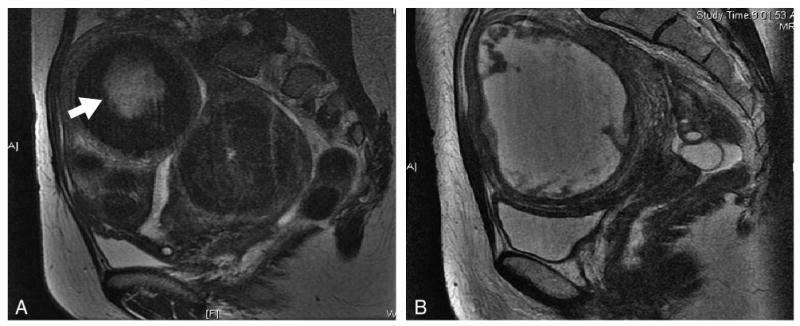
Degenerating leiomyomas seen on T2-weighted magnetic resonance imaging (MRI; A; arrow) and on T1-weighted MRI (B) with gadolinium contrast.
Similar articles
-
Pathologic features of uterine leiomyomas following uterine artery embolization.Int J Gynecol Pathol. 2001 Oct;20(4):407-9. doi: 10.1097/00004347-200110000-00017. Int J Gynecol Pathol. 2001. PMID: 11603229 No abstract available.
-
[Uterine leiomyoma and fibroleiomyoma: treatment for non-pregnant women ].Akush Ginekol (Sofiia). 2015;54 Suppl 1:3-18. Akush Ginekol (Sofiia). 2015. PMID: 26137765 Bulgarian. No abstract available.
-
Development of a Model for the Prediction of Treatment Response of Uterine Leiomyomas after Uterine Artery Embolization.Int J Med Sci. 2018 Nov 23;15(14):1771-1777. doi: 10.7150/ijms.28687. eCollection 2018. Int J Med Sci. 2018. PMID: 30588202 Free PMC article.
-
Uterine Artery Embolization of Uterine Leiomyomas: Predictive MRI Features of Volumetric Response.AJR Am J Roentgenol. 2021 Apr;216(4):967-974. doi: 10.2214/AJR.20.22906. Epub 2021 Feb 17. AJR Am J Roentgenol. 2021. PMID: 33594913
-
Bleeding associated with uterine leiomyomas. Tailor treatment to the individual patient.Prescrire Int. 2014 May;23(149):130-5. Prescrire Int. 2014. PMID: 24926520 Review.
Cited by
-
Clinical predictors of successful magnetic resonance-guided focused ultrasound (MRgFUS) for uterine leiomyoma.J Ther Ultrasound. 2013 Sep 2;1:15. doi: 10.1186/2050-5736-1-15. eCollection 2013. J Ther Ultrasound. 2013. PMID: 25512860 Free PMC article.
-
Vaginal Pessary for Uterine Repositioning during High-Intensity Focused Ultrasound Ablation of Uterine Leiomyomas.Gynecol Obstet Invest. 2016;81(3):285-8. doi: 10.1159/000441782. Epub 2015 Nov 20. Gynecol Obstet Invest. 2016. PMID: 26584482 Free PMC article.
-
Comparative Effectiveness of Uterine Leiomyoma Procedures Using a Large Insurance Claims Database.Obstet Gynecol. 2017 Nov;130(5):1047-1056. doi: 10.1097/AOG.0000000000002331. Obstet Gynecol. 2017. PMID: 29016510 Free PMC article.
-
Biomechanical Forces Determine Fibroid Stem Cell Transformation and the Receptivity Status of the Endometrium: A Critical Appraisal.Int J Mol Sci. 2022 Nov 17;23(22):14201. doi: 10.3390/ijms232214201. Int J Mol Sci. 2022. PMID: 36430682 Free PMC article. Review.
-
Putative human myometrial and fibroid stem-like cells have mesenchymal stem cell and endometrial stromal cell properties.Hum Reprod. 2020 Jan 1;35(1):44-57. doi: 10.1093/humrep/dez247. Hum Reprod. 2020. PMID: 31913469 Free PMC article.
References
-
- Speert H. Obstetrics and gynecology in America: a history. Chicago (IL): American College of Obstetricians and Gynecologists; 1980.
-
- Farquhar CM, Steiner CA. Hysterectomy rates in the United States 1990–1997. Obstet Gynecol. 2002;99:229–34. - PubMed
-
- Jacobson GF, Shaber RE, Armstrong MA, Hung YY. Hysterectomy rates for benign indications. Obstet Gynecol. 2006;107:1278–83. - PubMed
-
- Merrill RM. Hysterectomy surveillance in the United States, 1997 through 2005. Med Sci Monit. 2008;14:CR24–31. - PubMed
-
- Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188:100–7. - PubMed
Suggested Reading List
-
- Alternatives to hysterectomy in the management of leiomyomas. ACOG Practice Bulletin. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2008;112:387–400. - PubMed
-
- Catherino WH, editor. Insights and advances in uterine leiomyomas. New York (NY): Thieme; 2010. - PubMed
-
- Goodwin SC, Spies JB. Uterine fibroid embolization. N Engl J Med. 2009;361:690–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
