

First trimester uric acid and adverse pregnancy outcomes
- PMID: 21252861
- PMCID: PMC3062659
- DOI: 10.1038/ajh.2010.262
First trimester uric acid and adverse pregnancy outcomes
Abstract
Background: The association of elevated serum uric acid with the development of hypertension is established outside of pregnancy. We investigated whether first trimester uric acid was associated with the development of the following: gestational hypertension or pre eclampsia, these outcomes stratified by presence of hyperuricemia at delivery since this denotes more severe disease, preterm birth, or small for gestational age (SGA).
Methods: Uric acid was measured in 1,541 banked maternal plasma samples from a prior prospective cohort study that were collected at a mean gestational age of 9.0 (± 2.5) weeks. Polytomous regressions were performed and adjusted for parity and prepregnancy body mass index (BMI).
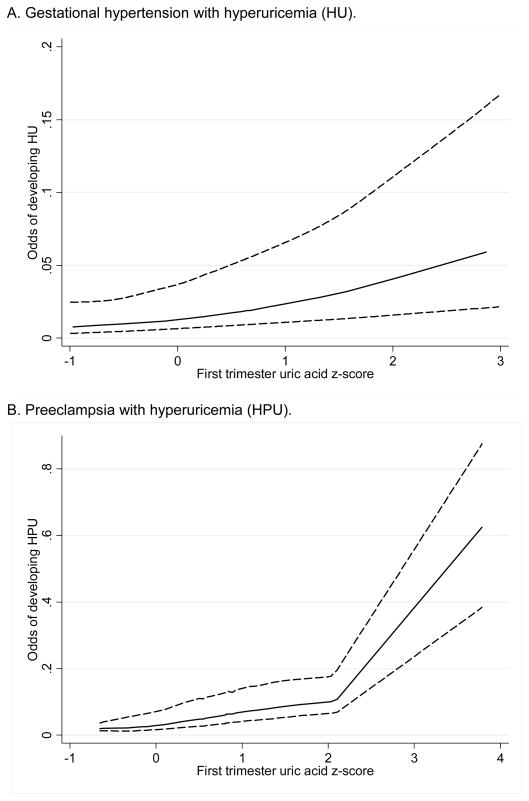
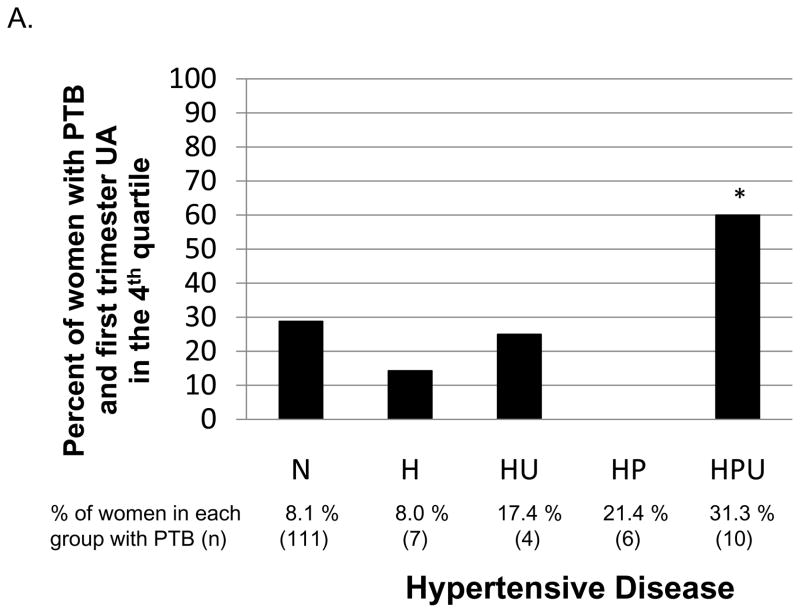
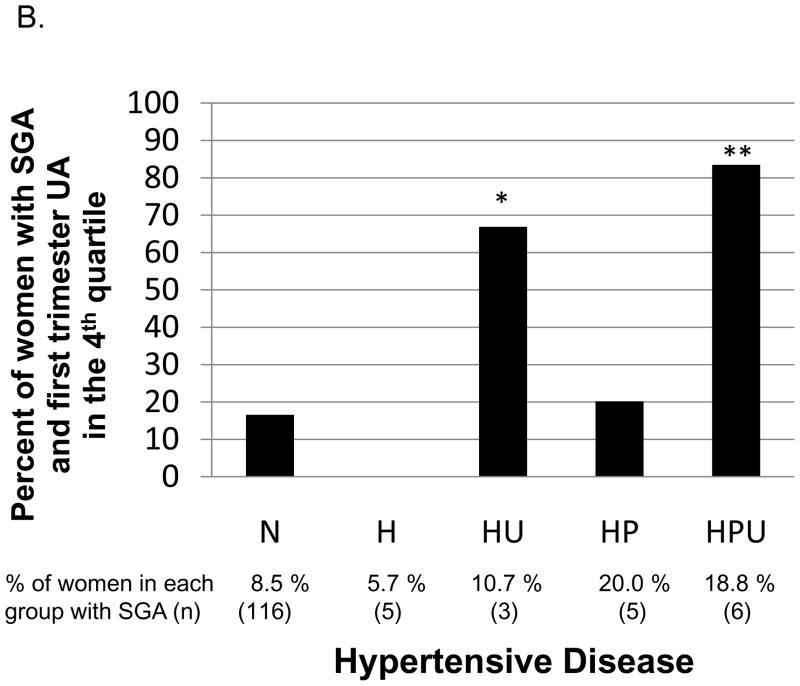
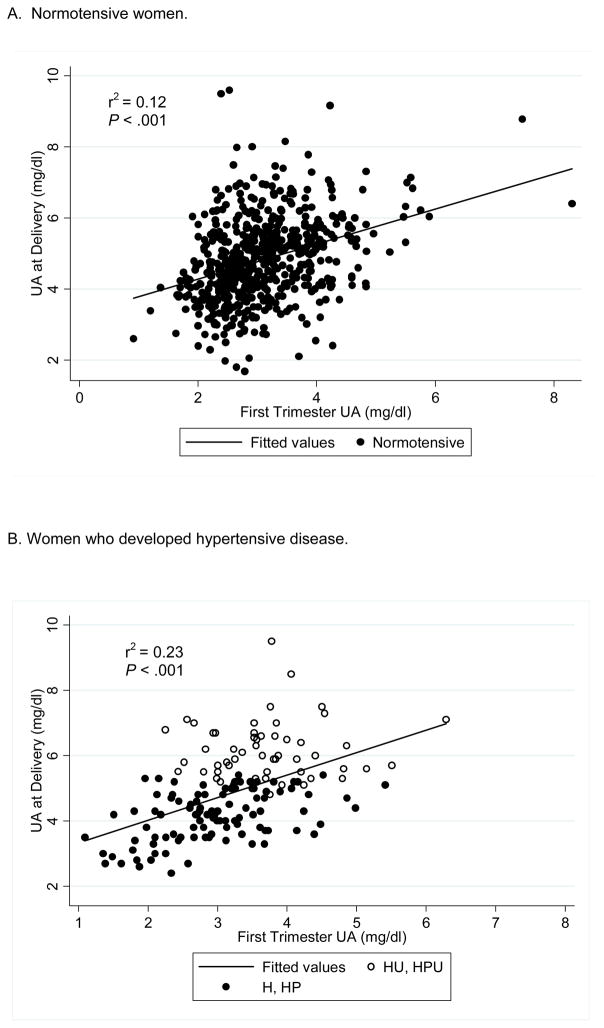
Results: First trimester uric acid in the highest quartile (>3.56 mg/dl) compared to lowest three quartiles was associated with an increased risk of developing pre-eclampsia (adjusted odds ratio (OR) = 1.82; 95% confidence interval (CI), 1.03-3.21) but not gestational hypertension. In women with hypertensive disease complicated by hyperuricemia at delivery, high first trimester uric acid was associated with a 3.22-fold increased risk of hyperuricemic gestational hypertension (HU) and a 3.65-fold increased risk of hyperuricemic pre-eclampsia (HPU). High first trimester uric acid was not associated with gestational hypertension or pre-eclampsia without hyperuricemia (H or HP) at delivery, preterm birth, or SGA. In women who developed hypertensive disease, elevated uric acid at delivery was only partly explained by elevated uric acid in the first trimester (r(2) = 0.23).
Conclusions: First trimester elevated uric acid was associated with later pre-eclampsia and more strongly with pre-eclampsia and gestational hypertension with hyperuricemia.
Conflict of interest statement
Figures
References
-
- Sibai BM, Gordon T, Thom E, Caritis SN, Klebanoff M, McNellis D, Paul RH. Risk factors for preeclampsia in healthy nulliparous women: a prospective multicenter study. The National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. American journal of obstetrics and gynecology. 1995;172(2 Pt 1):642–8. - PubMed
-
- Johnson RJ, Segal MS, Srinivas T, Ejaz A, Mu W, Roncal C, Sanchez-Lozada LG, Gersch M, Rodriguez-Iturbe B, Kang DH, Acosta JH. Essential hypertension, progressive renal disease, and uric acid: a pathogenetic link? J Am Soc Nephrol. 2005;16(7):1909–19. - PubMed
-
- Powers RW, Bodnar LM, Ness RB, Cooper KM, Gallaher MJ, Frank MP, Daftary AR, Roberts JM. Uric acid concentrations in early pregnancy among preeclamptic women with gestational hyperuricemia at delivery. American journal of obstetrics and gynecology. 2006;194(1):160. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
