

Clinical features and serum biomarkers in HIV immune reconstitution inflammatory syndrome after cryptococcal meningitis: a prospective cohort study
- PMID: 21253011
- PMCID: PMC3014618
- DOI: 10.1371/journal.pmed.1000384
Clinical features and serum biomarkers in HIV immune reconstitution inflammatory syndrome after cryptococcal meningitis: a prospective cohort study
Abstract
Background: Although antiretroviral therapy (ART) improves survival in persons with cryptococcal meningitis (CM) and AIDS, ART frequently elicits HIV immune reconstitution inflammatory syndrome (IRIS), an exaggerated and frequently deadly inflammatory reaction that complicates recovery from immunodeficiency. The pathogenesis of IRIS is poorly understood and prediction of IRIS is not possible.
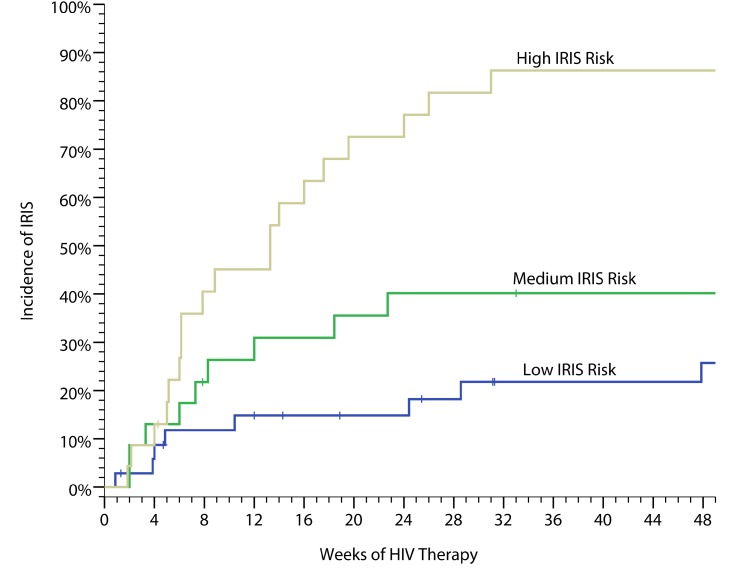
Methods and findings: We prospectively followed 101 ART-naïve Ugandans with AIDS and recent CM for one year after initiating ART, and used Luminex multiplex assays to compare serum cytokine levels in participants who did or did not develop IRIS. IRIS occurred in 45% of participants with recent CM on ART, including 30% with central nervous system (CNS) manifestations. The median time to CM-IRIS was 8.8 wk on ART. Overall mortality on ART was 36% with IRIS and 21% without IRIS. CM-IRIS was independently associated with death (HR = 2.3, 95% CI 1.1-5.1, p = 0.04). Patients experiencing subsequent CM-IRIS had 4-fold higher median serum cryptococcal antigen (CRAG) levels pre-ART (p = 0.006). Higher pre-ART levels of interleukin (IL)-4 and IL-17 as well as lower tumor necrosis factor (TNF)-α, granulocyte colony-stimulating factor (G-CSF), granulocyte-macrophage colony-stimulating factor (GM-CSF), and vascular endothelial growth factor (VEGF) predicted future IRIS in multivariate analyses (area under the curve [AUC] = 0.82). An algorithm based on seven pre-ART serum biomarkers was a robust tool for stratifying high (83%), moderate (48%), and low risk (23%) for IRIS in the cohort. After ART was initiated, increasing levels of C-reactive protein (CRP), D-dimer, IL-6, IL-7, IL-13, G-CSF, or IL-1RA were associated with increasing hazard of IRIS by time-to-event analysis (each p≤0.001). At the time of IRIS onset, multiple proinflammatory cytokine responses were present, including CRP and IL-6. Mortality was predicted by pre-ART increasing IL-17, decreasing GM-CSF, and CRP level >32 mg/l (highest quartile). Pre-ART CRP level >32 mg/l alone was associated with future death (OR = 8.3, 95% CI 2.7-25.6, p<0.001).
Conclusions: Pre-ART increases in Th(17) and Th(2) responses (e.g., IL-17, IL-4) and lack of proinflammatory cytokine responses (e.g., TNF-α, G-CSF, GM-CSF, VEGF) predispose individuals to subsequent IRIS, perhaps as biomarkers of immune dysfunction and poor initial clearance of CRAG. Although requiring validation, these biomarkers might be an objective tool to stratify the risk of CM-IRIS and death, and could be used clinically to guide when to start ART or use prophylactic interventions.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


 where:
where: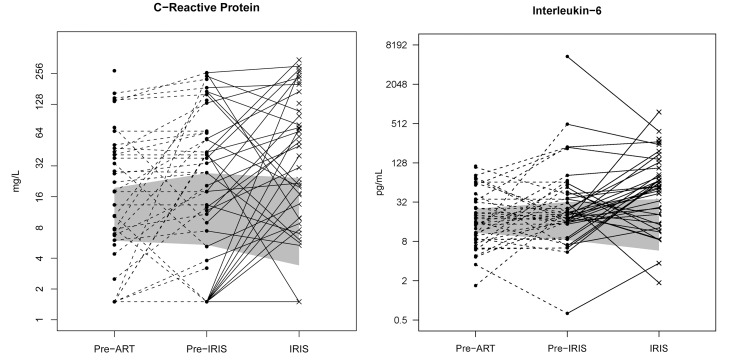

References
-
- French N, Gray K, Watera C, Nakiyingi J, Lugada E, et al. Cryptococcal infection in a cohort of HIV-1-infected Ugandan adults. AIDS. 2002;16:1031–1038. - PubMed
-
- Hakim JG, Gangaidzo IT, Heyderman RS, Mielke J, Mushangi E, et al. Impact of HIV infection on meningitis in Harare, Zimbabwe: a prospective study of 406 predominantly adult patients. AIDS. 2000;14:1401–1407. - PubMed
-
- Corbett EL, Churchyard GJ, Charalambos S, Samb B, Moloi V, et al. Morbidity and mortality in South African gold miners: impact of untreated disease due to human immunodeficiency virus. Clin Infect Dis. 2002;34:1251–1258. - PubMed
-
- Liechty CA, Solberg P, Were W, Ekwaru JP, Ransom RL, et al. Asymptomatic serum cryptococcal antigenemia and early mortality during antiretroviral therapy in rural Uganda. Trop Med Int Health. 2007;12:929–935. - PubMed
-
- Park BJ, Wannwmuehler KA, Marston BJ, Govender N, Pappas PG, et al. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23:525–530. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
