

Clinical application of optical coherence tomography for the imaging of non-melanocytic cutaneous tumors: a pilot multi-modal study
- PMID: 21254735
- PMCID: PMC3019059
Clinical application of optical coherence tomography for the imaging of non-melanocytic cutaneous tumors: a pilot multi-modal study
Erratum in
- J Med Life. 2011 Jan-Mar;4(1):7 p following 123
Abstract
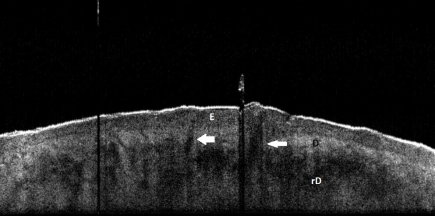
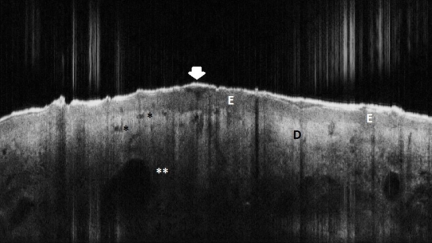
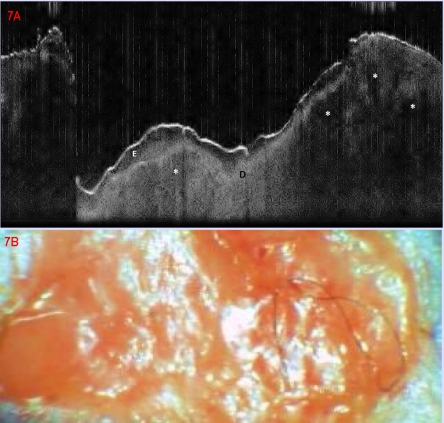
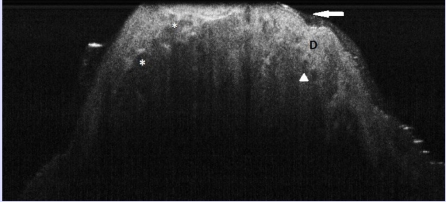
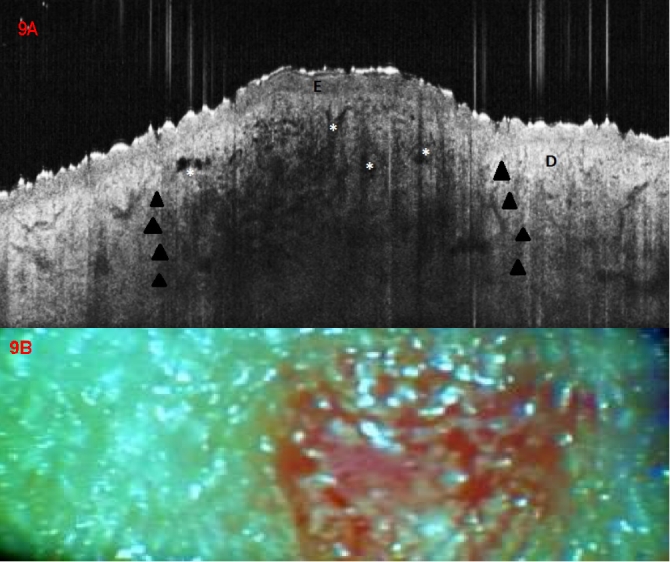
Context: Optical coherence tomography (OCT) is an emergent imaging technique, based on the interference of infrared radiation and living tissues, that allows the in vivo visualization of the skin structures, at high resolution and up to 1.6 mm depth. As such, there is mounting evidence that OCT may be an interesting technique for the diagnosis of skin diseases, including the noninvasive early detection of cutaneous tumors.
Objective: We aimed to investigate the utility of OCT for the diagnosis of non-melanocytic, non-pigmented cutaneous tumors.
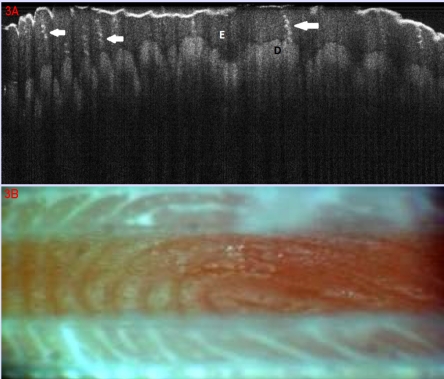
Methods: Preliminary results are presented from an initiated study. Fifteen consecutive patients with clinical suspicion of epithelial cancers and precancers registered over one week in a university dermatologic department were included. As control were selected 7 patients with inflammatory skin diseases (psoriasis, lichen planus, cutaneous lupus erythematosus). In all study and control patients, the lesions and samples of normal, perilesional skin were documented by clinical digital photography, contact dermoscopy with digital image capture and OCT with central wavelength of 930 nm. Final diagnosis was certified by histopathological analysis.
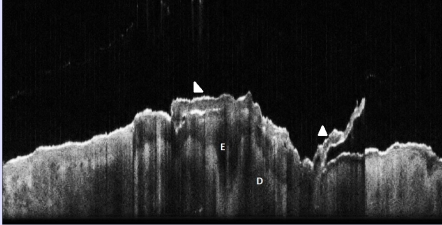
Results: We could identify morphological features in OCT examination that distinguished between normal and lesional skin, and between neoplastic vs. inflammatory lesions. In the same time, combining OCT and dermatoscopical evaluation of a lesion improved the performance of diagnosis when compared to clinical diagnosis alone and with either OCT or dermoscopy imaging used alone.
Conclusions: OCT appears as a promising method of in vivo diagnosis of early neoplastic cutaneous lesions with equivocal clinical and/or dermoscopic aspect. Continuation of our study as well as other larger investigation will be able to contribute with new insights in the role of OCT in the non-invasive diagnosis of skin disease.
Figures





References
-
- Andersen P. Handbook of Non–Invasive Methods and the Skin. Florida: Boca Raton; 1996. Optical coherence tomography in dermatology.
-
- Welzel J. Optical coherence tomography in dermatology: a review. Skin Res Technol . 2001;7:1–9. - PubMed
-
- Tadrous PJ. Methods for imaging the structure and function of living tissues and cells: optical coherence tomography. J Pathol . 2000;(191):115–119. - PubMed
-
- Fujimoto JG. Optical biopsy and imaging using optical coherence tomography. Nat Med. 1995;1:970–972. - PubMed
-
- Welzel J, Lankenau E. Optical coherence tomography of the human skin . J Am Acad Dermatol. 1997;37:958–963. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials