

Fucosyltransferase 2 non-secretor and low secretor status predicts severe outcomes in premature infants
- PMID: 21256510
- PMCID: PMC3412418
- DOI: 10.1016/j.jpeds.2010.10.043
Fucosyltransferase 2 non-secretor and low secretor status predicts severe outcomes in premature infants
Abstract
Objective: To investigate secretor gene fucosyltransferase 2 (FUT2) polymorphism and secretor phenotype in relation to outcomes of prematurity.
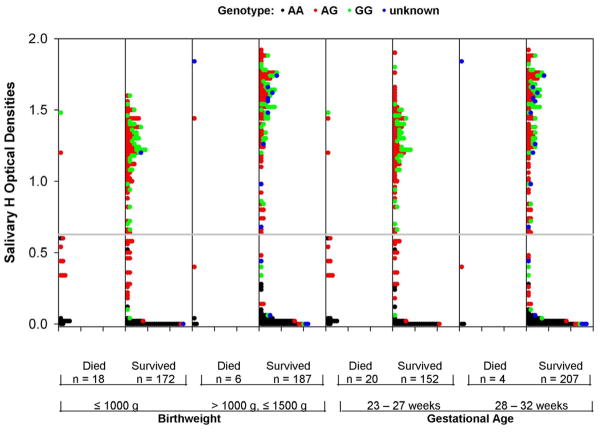
Study design: Study infants were ≤32 weeks gestational age. Secretor genotype was determined from salivary DNA. Secretor phenotype was measured with H antigen, the carbohydrate produced by secretor gene enzymes, in saliva samples collected on day 9 ± 5. The optimal predictive cutoff point in salivary H values was identified with Classification and Regression Tree analysis. Study outcomes were death, necrotizing enterocolitis (NEC, Bell's stage II/III), and confirmed sepsis.
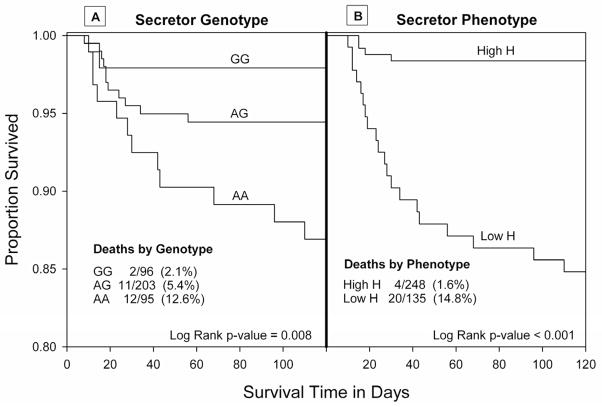
Results: There were 410 study infants, 26 deaths, 30 cases of NEC, and 96 cases of sepsis. Analyzed by genotype, 13% of 95 infants who were non-secretors, 5% of 203 infants who were heterozygotes, and 2% of 96 infants who were secretor dominant died (P = .01). Analyzed by phenotype, 15% of 135 infants with low secretor phenotype died, compared with 2% of 248 infants with high secretor phenotype (predictive value = 76%, P < .001). Low secretor phenotype was associated (P < .05) with NEC, and non-secretor genotype was associated (P = .05) with gram negative sepsis. Secretor status remained significant after controlling for multiple clinical factors.
Conclusions: Secretor genotype and phenotype may provide strong predictive biomarkers of adverse outcomes in premature infants.
Copyright © 2011 Mosby, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Callaghan WM, MacDorman MF, Rasmussen SA, Qin C, Lackritz EM. The contribution of preterm birth to infant mortality rates in the United States. Pediatrics. 2006;118(4):1566–1573. - PubMed
-
- Fanaroff AA, Stoll BJ, Wright LL, et al. Trends in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet Gynecol. 2007;196(2):147, e141–148. - PubMed
-
- Ambalavanan N, Carlo WA, Bobashev G, et al. Prediction of death for extremely low birth weight neonates. Pediatrics. 2005;116(6):1367–1373. - PubMed
-
- Hussain F, Gilshenan K, Gray PH. Does lactate level in the first 12 hours of life predict mortality in extremely premature infants? J Paediatr Child Health. 2009;45(5):263–267. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
