

A simple strategy improves prehospital electrocardiogram utilization and hospital treatment for patients with acute coronary syndrome (from the ST SMART Study)
- PMID: 21256997
- PMCID: PMC5599262
- DOI: 10.1016/j.amjcard.2010.09.027
A simple strategy improves prehospital electrocardiogram utilization and hospital treatment for patients with acute coronary syndrome (from the ST SMART Study)
Abstract
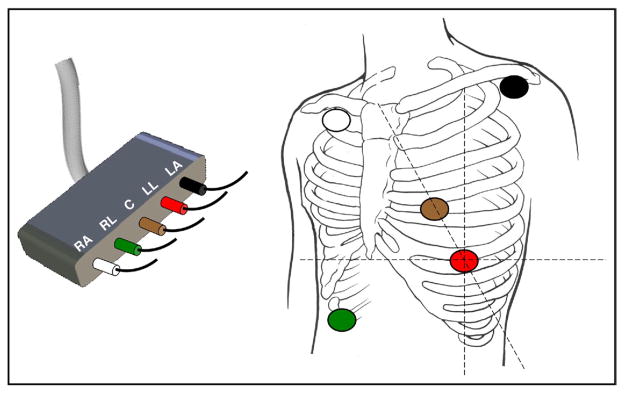
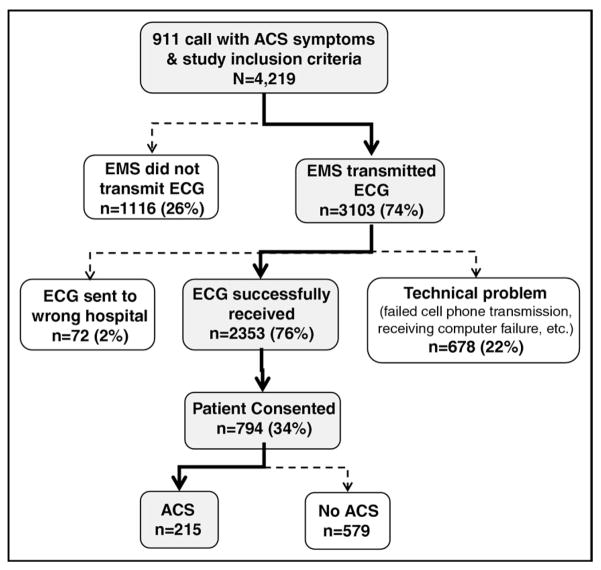
Although the American Heart Association recommends a prehospital electrocardiogram (ECG) be recorded for all patients who access the emergency medical system with symptoms of acute coronary syndrome (ACS), widespread use of prehospital ECG has not been achieved in the United States. A 5-year prospective randomized clinical trial was conducted in a predominately rural county in northern California to test a simple strategy for acquiring and transmitting prehospital ECGs that involved minimal paramedic training and decision making. A 12-lead ECG was synthesized from 5 electrodes and continuous ST-segment monitoring was performed with ST-event ECGs automatically transmitted to the destination hospital emergency department. Patients randomized to the experimental group had their ECGs printed out in the emergency department with an audible voice alarm, whereas control patients had an ECG after hospital arrival, as was the standard of care in the county. The result was that nearly 3/4 (74%) of 4,219 patients with symptoms of ACS over the 4-year study enrollment period had a prehospital ECG. Mean time from 911 call to first ECG was 20 minutes in those with a prehospital ECG versus 79 minutes in those without a prehospital ECG (p <0.0001). Mean paramedic scene time in patients with a prehospital ECG was just 2 minutes longer than in those without a prehospital ECG (95% confidence interval 1.2 to 3.6, p <0.001). Patients with non-ST-elevation myocardial infarction or unstable angina pectoris had a faster time to first intravenous drug and there was a suggested trend for a faster door-to-balloon time and lower risk of mortality in patients with ST-elevation myocardial infarction. In conclusion, increased paramedic use of prehospital ECGs and decreased hospital treatment times for ACS are feasible with a simple approach tailored to characteristics of a local geographic region.
Copyright © 2011 Elsevier Inc. All rights reserved.
Figures
References
-
- Diercks DB, Kontos MC, Chen AY, Pollack CV, Wiviott SD, Rumsfeld JS, Magid DJ, Gibler WB, Cannon CP, Peterson ED, Roe MT. Utilization and impact of pre-hospital electrocardiograms for patients with acute ST-segment elevation myocardial infarction. Data from the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network Registry. J Am Coll Cardiol. 2009;53:161–166. - PubMed
-
- Drew BJ, Dempsey ED, Joo TH, Sommargren CE, Glancy JP, Benedick K, Krucoff MW. Pre-hospital synthesized 12-lead ECG ischemia monitoring with trans-telephonic transmission in acute coronary syndromes: pilot study results of the ST SMART trial. J Electrocardiol. 2004;37:214–221. - PubMed
-
- Cannon CP, Battler A, Brindis RG, Cox JL, Ellis SG, Every NR, Flaherty JT, Harrington RA, Krumholz HM, Simoons ML, Van de Werf FJJ, Weintraub WS. American College of Cardiology key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes. J Am Coll Cardiol. 2001;38:2114–2130. - PubMed
-
- Thygesen K, Alpert JS, White HD Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50:2173–2195. - PubMed
-
- ACC/AHA 2007 guidelines for the management of patients with unstable angina/non–ST-elevation myocardial infarction. Circulation. 2007;116(suppl):e148–e304. - PubMed
