

Predicting the risk for dialysis or death in IgA nephropathy
- PMID: 21258035
- PMCID: PMC3065230
- DOI: 10.1681/ASN.2010040355
Predicting the risk for dialysis or death in IgA nephropathy
Abstract
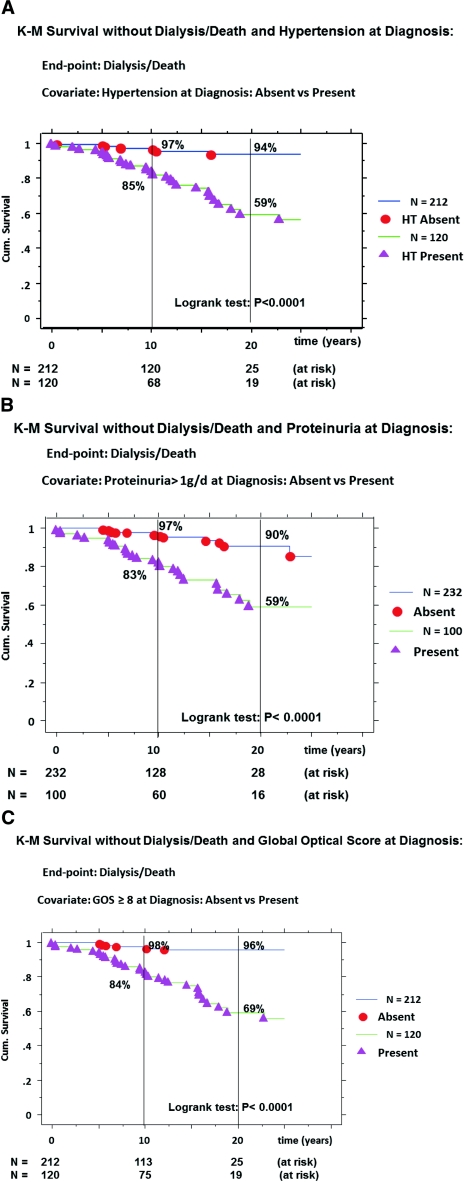
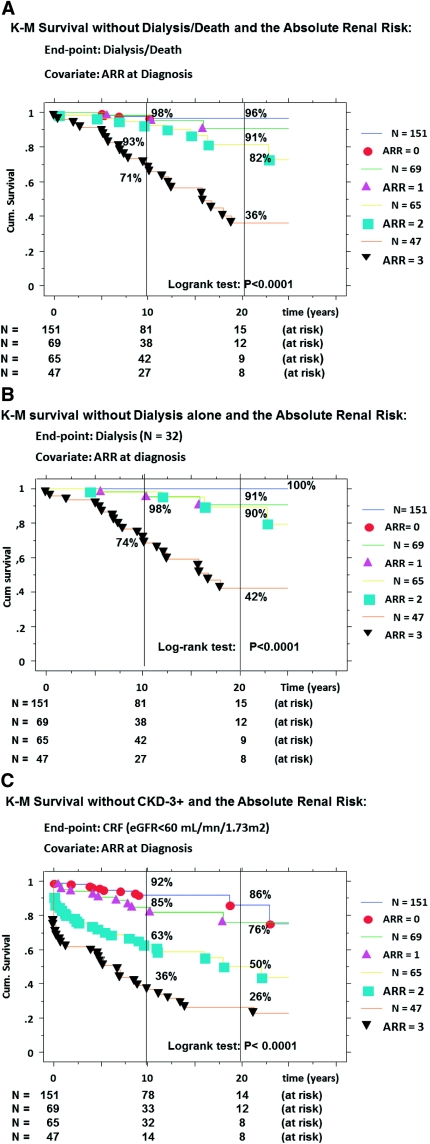
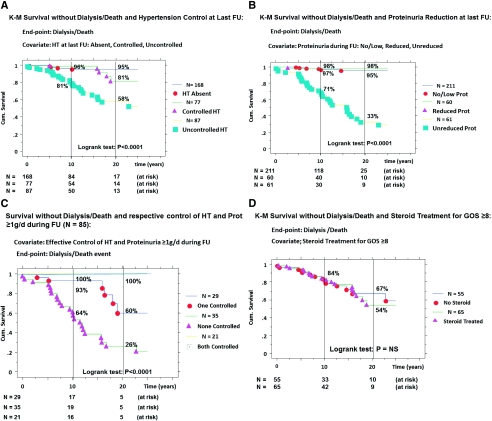
For the individual patient with primary IgA nephropathy (IgAN), it remains a challenge to predict long-term outcomes for patients receiving standard treatment. We studied a prospective cohort of 332 patients with biopsy-proven IgAN patients followed over an average of 13 years. We calculated an absolute renal risk (ARR) of dialysis or death by counting the number of risk factors present at diagnosis: hypertension, proteinuria ≥1 g/d, and severe pathologic lesions (global optical score, ≥8). Overall, the ARR score allowed significant risk stratification (P < 0.0001). The cumulative incidence of death or dialysis at 10 and 20 years was 2 and 4%, respectively, for ARR=0; 2 and 9% for ARR=1; 7 and 18% for ARR=2; and 29 and 64% for ARR=3, in adequately treated patients. When achieved, control of hypertension and reduction of proteinuria reduced the risk for death or dialysis. In conclusion, the absolute renal risk score, determined at diagnosis, associates with risk for dialysis or death.
Copyright © 2011 by the American Society of Nephrology
Figures
References
-
- Berger J, Hinglais N: Intercapillary deposits of IgA-IgG. J Urol Nephrol 74: 694–695, 1968 - PubMed
-
- Berger J: IgA glomerular deposits in renal disease. Transplant Proc 1: 939–944, 1969 - PubMed
-
- Donadio JV, Grande JP: IgA nephropathy. N Engl J Med 347: 738–748, 2002 - PubMed
-
- Barratt J, Feehally J. IgA nephropathy. J Am Soc Nephrol 16: 2088–2097, 2005 - PubMed
-
- Berthoux FC, Mohey H, Afiani A: Natural history of primary IgA nephropathy. Semin Nephrol 28: 4–9, 2008 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
