

TRPC6 enhances angiotensin II-induced albuminuria
- PMID: 21258036
- PMCID: PMC3060446
- DOI: 10.1681/ASN.2010050522
TRPC6 enhances angiotensin II-induced albuminuria
Abstract
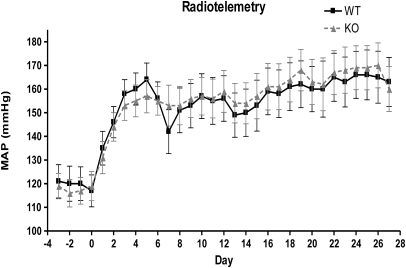
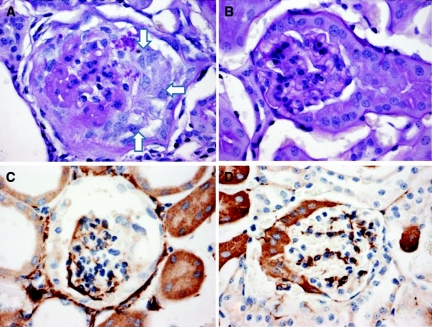
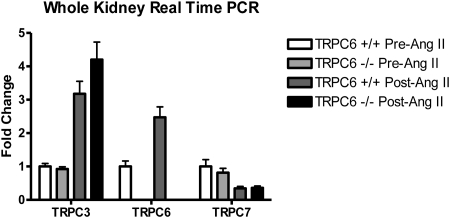
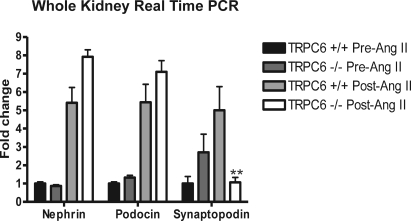
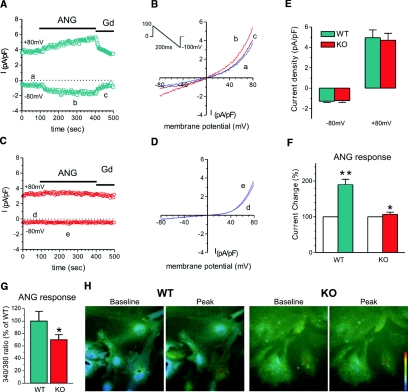
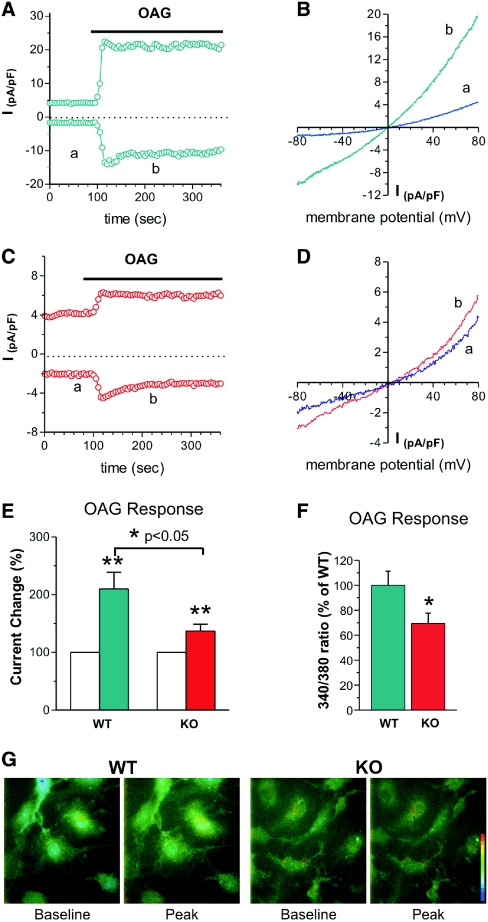
Mutations in the canonical transient receptor potential cation channel 6 (TRPC6) are responsible for familial forms of adult onset focal segmental glomerulosclerosis (FSGS). The mechanisms by which TRPC6 mutations cause kidney disease are not well understood. We used TRPC6-deficient mice to examine the function of TRPC6 in the kidney. We found that adult TRPC6-deficient mice had BP and albumin excretion rates similar to wild-type animals. Glomerular histomorphology revealed no abnormalities on both light and electron microscopy. To determine whether the absence of TRPC6 would alter susceptibility to hypertension and renal injury, we infused mice with angiotensin II continuously for 28 days. Although both groups developed similar levels of hypertension, TRPC6-deficient mice had significantly less albuminuria, especially during the early phase of the infusion; this suggested that TRPC6 adversely influences the glomerular filter. We used whole-cell patch-clamp recording to measure cell-membrane currents in primary cultures of podocytes from both wild-type and TRPC6-deficient mice. In podocytes from wild-type mice, angiotensin II and a direct activator of TRPC6 both augmented cell-membrane currents; TRPC6 deficiency abrogated these increases in current magnitude. Our findings suggest that TRPC6 promotes albuminuria, perhaps by promoting angiotensin II-dependent increases in Ca(2+), suggesting that TRPC6 blockade may be therapeutically beneficial in proteinuric kidney disease.
Figures

References
-
- Dietrich A, Kalwa H, Rost BR, Gudermann T: The diacylgylcerol-sensitive TRPC3/6/7 subfamily of cation channels: Functional characterization and physiological relevance. Pflugers Arch 451: 72–80, 2005 - PubMed
-
- Winn MP, Conlon PJ, Lynn KL, Farrington MK, Creazzo T, Hawkins AF, Daskalakis N, Kwan SY, Ebersviller S, Burchette JL, Pericak-Vance MA, Howell DN, Vance JM, Rosenberg PB: A mutation in the TRPC6 cation channel causes familial focal segmental glomerulosclerosis. Science 308: 1801–1804, 2005 - PubMed
-
- Kestila M, Lenkkeri U, Mannikko M, Lamerdin J, McCready P, Putaala H, Ruotsalainen V, Morita T, Nissinen M, Herva R, Kashtan CE, Peltonen L, Holmberg C, Olsen A, Tryggvason K: Positionally cloned gene for a novel glomerular protein–nephrin–is mutated in congenital nephrotic syndrome. Mol Cell 1: 575–582, 1998 - PubMed
-
- Boute N, Gribouval O, Roselli S, Benessy F, Lee H, Fuchshuber A, Dahan K, Gubler MC, Niaudet P, Antignac C: NPHS2, encoding the glomerular protein podocin, is mutated in autosomal recessive steroid-resistant nephrotic syndrome. Nat Genet 24: 349–354, 2000 - PubMed
-
- Shankland SJ: The podocyte's response to injury: Role in proteinuria and glomerulosclerosis. Kidney Int 69: 2131–2147, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
