

Living and dying with severe chronic obstructive pulmonary disease: multi-perspective longitudinal qualitative study
- PMID: 21262897
- PMCID: PMC3025692
- DOI: 10.1136/bmj.d142
Living and dying with severe chronic obstructive pulmonary disease: multi-perspective longitudinal qualitative study
Abstract
Objectives: To understand the perspectives of people with severe chronic obstructive pulmonary disease (COPD) as their illness progresses, and of their informal and professional carers, to inform provision of care for people living and dying with COPD.
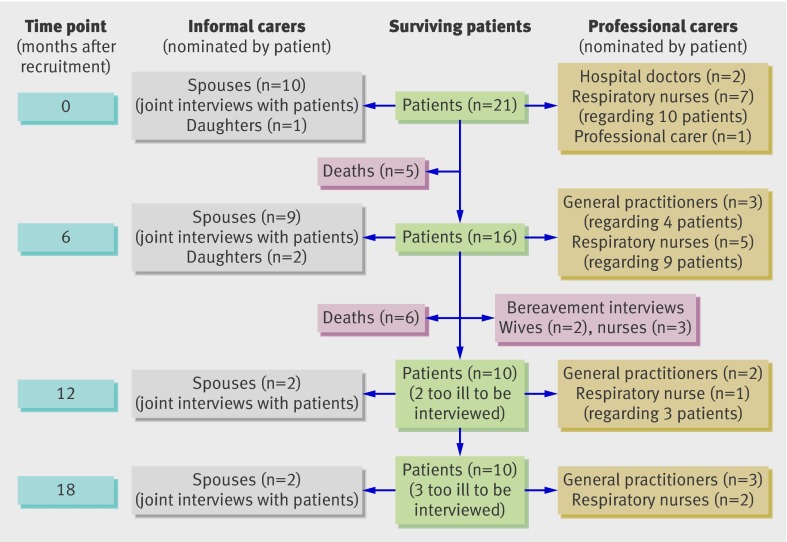
Design: Up to four serial qualitative interviews were conducted with each patient and nominated carer over 18 months. Interviews were transcribed and analysed both thematically and as narratives.
Participants: 21 patients, and 13 informal carers (a family member, friend, or neighbour) and 18 professional carers (a key health or social care professional) nominated by the patients.
Setting: Primary and secondary care in Lothian, Tayside, and Forth Valley, Scotland, during 2007-9.
Results: Eleven patients died during the study period. Our final dataset comprised 92 interviews (23 conducted with patient and informal carer together). Severe symptoms that caused major disruption to normal life were described, often in terms implying acceptance of the situation as a "way of life" rather than an "illness." Patients and their informal carers adapted to and accepted the debilitating symptoms of a lifelong condition. Professional carers' familiarity with the patients' condition, typically over many years, and prognostic uncertainty contributed to the difficulty of recognising and actively managing end stage disease. Overall, patients told a "chaos narrative" of their illness that was indistinguishable from their life story, with no clear beginning and an unanticipated end described in terms comparable with attitudes to death in a normal elderly population.
Conclusions: Our findings challenge current assumptions underpinning provision of end of life care for people with COPD. The policy focus on identifying a time point for transition to palliative care has little resonance for people with COPD or their clinicians and is counter productive if it distracts from early phased introduction of supportive care. Careful assessment of possible supportive and palliative care needs should be triggered at key disease milestones along a lifetime journey with COPD, in particular after hospital admission for an exacerbation.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Republished in
-
Living and dying with severe chronic obstructive pulmonary disease: multi-perspective longitudinal qualitative study.BMJ Support Palliat Care. 2011 Sep;1(2):174-83. doi: 10.1136/bmjspcare.d142rep. BMJ Support Palliat Care. 2011. PMID: 24653231
Comment in
-
Living and dying with COPD. End of life trajectories across conditions.BMJ. 2011 Feb 15;342:d989. doi: 10.1136/bmj.d989. BMJ. 2011. PMID: 21324999 No abstract available.
-
Living and dying with COPD. What happens in neurological disease.BMJ. 2011 Feb 15;342:d994. doi: 10.1136/bmj.d994. BMJ. 2011. PMID: 21325000 No abstract available.
References
-
- Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet 2007;370:765-73. - PubMed
-
- NHS End of Life Care Programme. The gold standards framework. 2010. www.goldstandardsframework.nhs.uk.
-
- Centers for Medicare & Medicaid Services. Publication no 02154: a special way of caring for people who are terminally ill. US Department of Health and Human Services, 2008.
-
- Department of Health. NHS end of life care strategy: promoting high quality care for all adults at the end of life. Department of Health, 2008.
-
- World Health Organization. The solid facts: palliative care. WHO, 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical