

High survival rate after two-stage resection of advanced colorectal liver metastases: response-based selection and complete resection define outcome
- PMID: 21263087
- PMCID: PMC3068054
- DOI: 10.1200/JCO.2010.32.6132
High survival rate after two-stage resection of advanced colorectal liver metastases: response-based selection and complete resection define outcome
Abstract
Purpose: Prolonged survival after two-stage resection (TSR) of advanced colorectal liver metastases (CLM) may be the result of selection of best responders to chemotherapy. The impact of complete resection in this well-selected group is controversial.
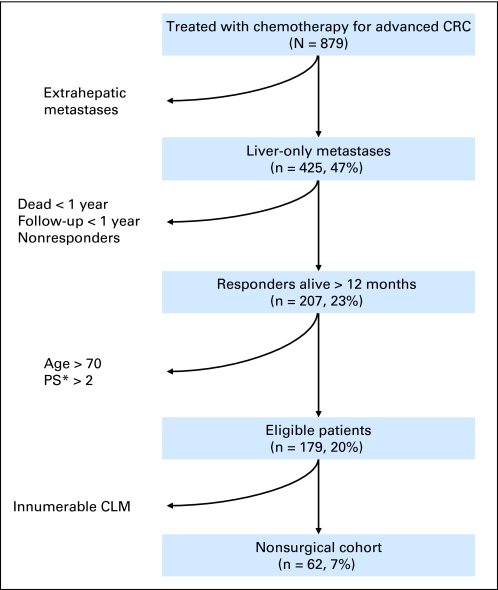
Patients and methods: Data on 890 patients undergoing resection and 879 patients who received only chemotherapy for CLM were collected prospectively. We used intent-to-treat analysis to evaluate the survival of patients who underwent TSR. Additionally, we evaluated a cohort of nonsurgically treated patients selected to mirror the TSR population: colorectal metastases with liver-only disease, objective response to chemotherapy, and alive 1 year after chemotherapy initiation.
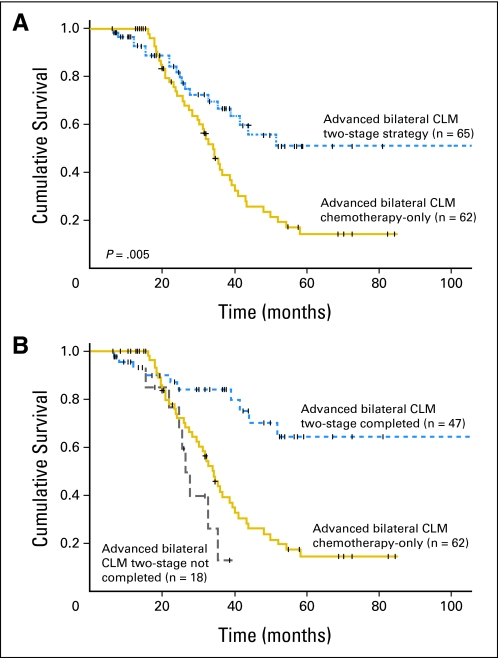
Results: Sixty-five patients underwent the first stage of TSR; 62 patients fulfilled the inclusion criteria for the medical group. TSR patients had a mean of 6.7 ± 3.4 CLM with mean size of 4.5 ± 3.1 cm. Nonsurgical patients had a mean of 5.9 ± 2.9 CLM with mean size of 5.4 ± 3.4 cm (not significant). Forty-seven TSR patients (72%) completed the second stage. Progression between stages was the main cause of noncompletion of the second stage (61%). After 50 months median follow-up, the 5-year survival rate was 51% in the TSR group and 15% in the medical group (P = .005). In patients who underwent TSR, noncompletion of TSR and major postoperative complications were independently associated with worse survival.
Conclusion: TSR is associated with excellent outcome in patients with advanced CLM as a result of both selection by chemotherapy and complete resection of metastatic disease.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Advanced colorectal liver metastases and surgery after preoperative chemotherapy: is response-based selection enough?J Clin Oncol. 2011 Jul 1;29(19):2733-4; author reply 2734-5. doi: 10.1200/JCO.2011.35.9976. Epub 2011 May 23. J Clin Oncol. 2011. PMID: 21606418 No abstract available.
References
-
- Scheele J, Stang R, Altendorf-Hofmann A, et al. Resection of colorectal liver metastases. World J Surg. 1995;19:59–71. - PubMed
-
- Blazer DG, 3rd, Kishi Y, Maru DM, et al. Pathologic response to preoperative chemotherapy: A new outcome end point after resection of hepatic colorectal metastases. J Clin Oncol. 2008;26:5344–5351. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
