

Phase III trial of weekly methotrexate or pulsed dactinomycin for low-risk gestational trophoblastic neoplasia: a gynecologic oncology group study
- PMID: 21263100
- PMCID: PMC3068058
- DOI: 10.1200/JCO.2010.30.4386
Phase III trial of weekly methotrexate or pulsed dactinomycin for low-risk gestational trophoblastic neoplasia: a gynecologic oncology group study
Abstract
Purpose: There is no consensus on the best regimen for the primary treatment of low-risk gestational trophoblastic neoplasia (GTN).
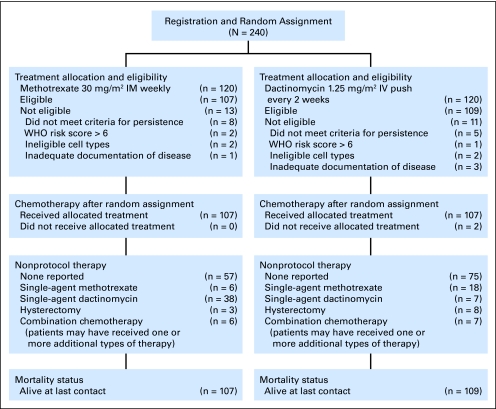
Patients and methods: Two commonly used single-drug regimens were compared with respect to the proportion of patients meeting the criteria for a complete response (CR) in a randomized phase III trial conducted by the Gynecologic Oncology Group. Eligibility was purposefully broad to maximize the generalizability of the results and included patients with a WHO risk score of 0 to 6 and patients with metastatic disease (limited to lung lesions < 2 cm, adnexa, or vagina) or choriocarcinoma.
Results: Two hundred forty women were enrolled, and 216 were deemed eligible. Biweekly intravenous dactinomycin 1.25 mg/m² was statistically superior to weekly intramuscular (IM) methotrexate 30 mg/m² (CR: 70% v 53%; P = .01). Similarly, in patients with low-risk GTN as defined before the 2002 WHO risk score revisions (risk score of 0 to 4 and excluding choriocarcinoma), response was 58% and 73% in the methotrexate and dactinomycin arms, respectively (P = .03). Both regimens were less effective if the WHO risk score was 5 or 6 or if the diagnosis was choriocarcinoma (CR: 9% and 42%, respectively). There were two potential recurrences; one at 4 months (dactinomycin) and one at 22 months (methotrexate). Not all patients completed follow-up. Both regimens were well tolerated.
Conclusion: The biweekly dactinomycin regimen has a higher CR rate than the weekly IM methotrexate regimen in low-risk GTN, a generally curable disease.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Treatment of low-risk gestational trophoblastic neoplasia.J Clin Oncol. 2011 Mar 1;29(7):786-8. doi: 10.1200/JCO.2010.31.0151. Epub 2011 Jan 24. J Clin Oncol. 2011. PMID: 21263092 No abstract available.
References
-
- Rustin GJ, Newlands ES, Lutz JM, et al. Combination but not single-agent methotrexate chemotherapy for gestational trophoblastic tumors increases the incidence of second tumors. J Clin Oncol. 1996;14:2769–2773. - PubMed
-
- Lurain JR, Elfstrand EP. Single-agent methotrexate chemotherapy for the treatment of nonmetastatic trophoblastic tumors. Am J Obstet Gynecol. 1995;172:574–579. - PubMed
-
- Roberts JP, Lurain JR. Treatment of low-risk metastatic gestational trophoblastic tumors with single-agent chemotherapy. Am J Obstet Gynecol. 1996;174:1917–1923. discussion 1923–1924. - PubMed
-
- Soper JT, Clarke-Pearson DL, Berchuck A, et al. 5-day methotrexate for women with metastatic gestational trophoblastic disease. Gynecol Oncol. 1994;54:76–79. - PubMed
-
- Elit L, Covens A, Osborne R, et al. High-dose methotrexate for gestational trophoblastic disease. Gynecol Oncol. 1994;54:282–287. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
