

Ambulatory blood pressure monitoring in 9357 subjects from 11 populations highlights missed opportunities for cardiovascular prevention in women
- PMID: 21263119
- PMCID: PMC8377766
- DOI: 10.1161/HYPERTENSIONAHA.110.156828
Ambulatory blood pressure monitoring in 9357 subjects from 11 populations highlights missed opportunities for cardiovascular prevention in women
Abstract
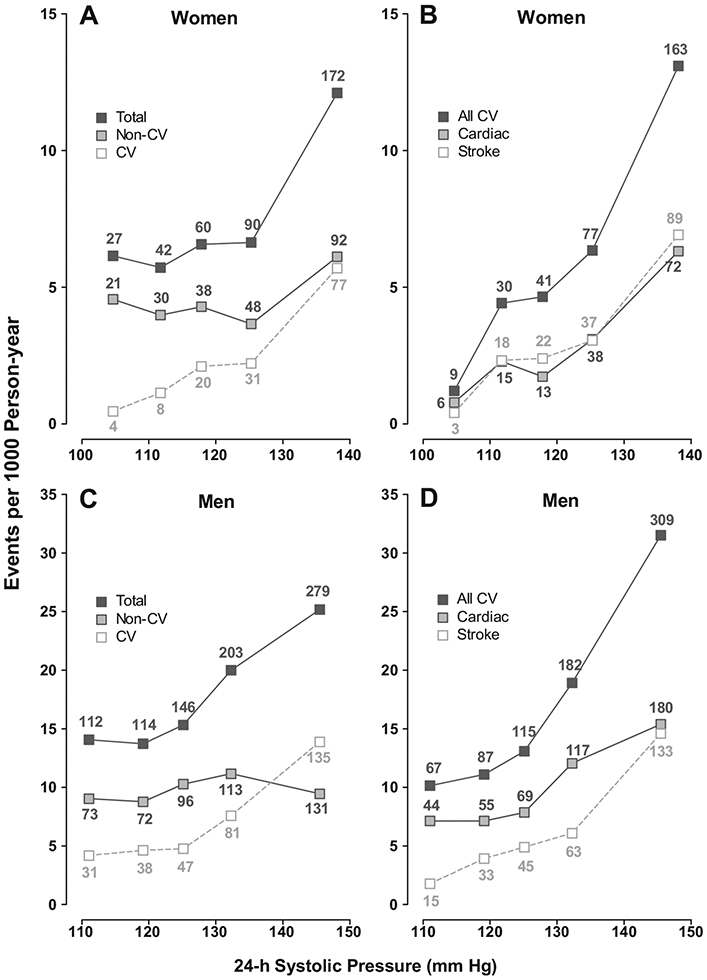
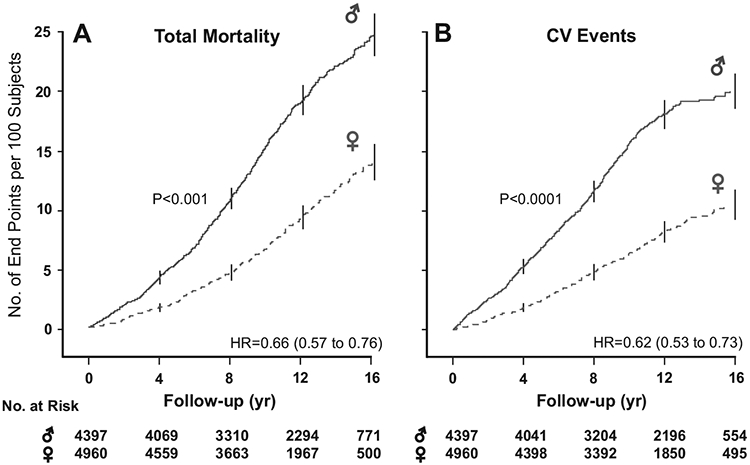
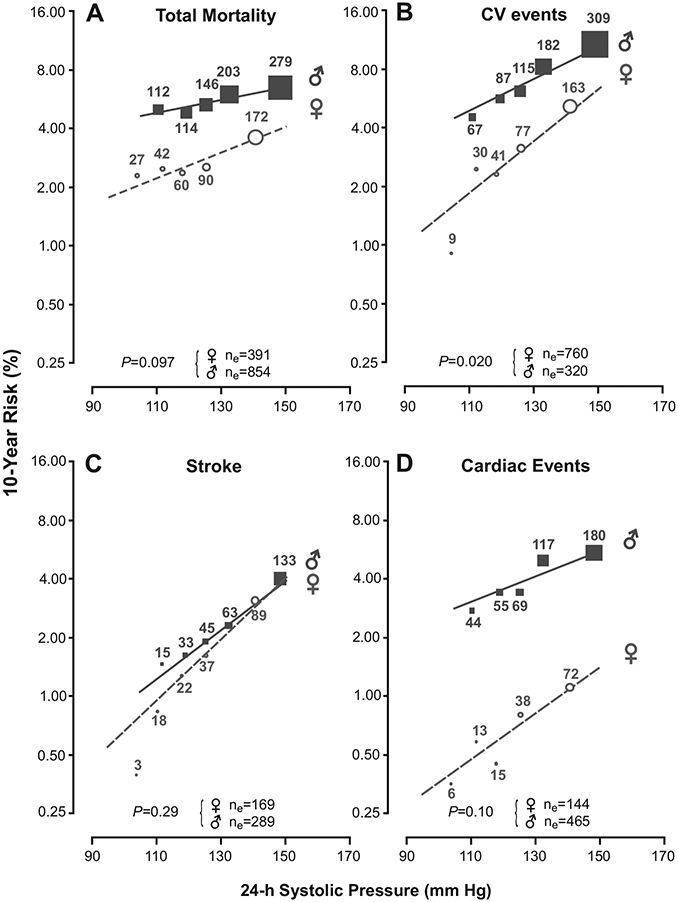
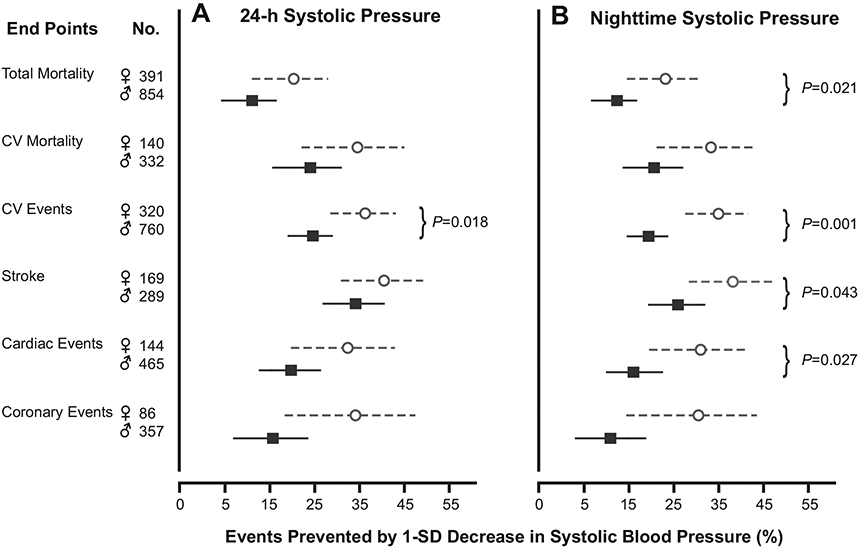
To analyze sex-specific relative and absolute risks associated with blood pressure (BP), we performed conventional and 24-hour ambulatory BP measurements in 9357 subjects (mean age, 52.8 years; 47% women) recruited from 11 populations. We computed standardized multivariable-adjusted hazard ratios for associations between outcome and systolic BP. During a course of 11.2 years (median), 1245 participants died, 472 of cardiovascular causes. The number of fatal combined with nonfatal events was 1080, 525, and 458 for cardiovascular and cardiac events and for stroke, respectively. In women and men alike, systolic BP predicted outcome, irrespective of the type of BP measurement. Women compared with men were at lower risk (hazard ratios for death and all cardiovascular events=0.66 and 0.62, respectively; P<0.001). However, the relation of all cardiovascular events with 24-hour BP (P=0.020) and the relations of total mortality (P=0.023) and all cardiovascular (P=0.0013), cerebrovascular (P=0.045), and cardiac (P=0.034) events with nighttime BP were steeper in women than in men. Consequently, per a 1-SD decrease, the proportion of potentially preventable events was higher in women than in men for all cardiovascular events (35.9% vs 24.2%) in relation to 24-hour systolic BP (1-SD, 13.4 mm Hg) and for all-cause mortality (23.1% vs 12.3%) and cardiovascular (35.1% vs 19.4%), cerebrovascular (38.3% vs 25.9%), and cardiac (31.0% vs 16.0%) events in relation to systolic nighttime BP (1-SD, 14.1 mm Hg). In conclusion, although absolute risks associated with systolic BP were lower in women than men, our results reveal a vast and largely unused potential for cardiovascular prevention by BP-lowering treatment in women.
Figures
Comment in
-
Ambulatory blood pressure monitoring to assess cardiovascular risk in women.Hypertension. 2011 Mar;57(3):377-8. doi: 10.1161/HYPERTENSIONAHA.110.158295. Epub 2011 Jan 24. Hypertension. 2011. PMID: 21263122 No abstract available.
-
Referral of women to ambulatory blood pressure monitoring.Hypertension. 2011 Jun;57(6):e26; author reply e27. doi: 10.1161/HYPERTENSIONAHA.111.172759. Epub 2011 Apr 25. Hypertension. 2011. PMID: 21518962 No abstract available.
References
-
- Mosca L, Appel LJ, Benjamin EJ, Berra K, Chandra-Strobos N, Fabunmi RP, Grady D, Haan CK, Hayes SN, Judelson DR, Keenan NL, McBride P, Oparil S, Ouyang P, Oz MC, Mendelsohn ME, Pasternak RC, Pinn VW, Robertson RM, Schenck-Gustafsson K, Sila CA, Smith SC Jr, Sopko G, Taylor AL, Walsh BW, Wenger NK, Williams CL. Evidence-based guidelines for cardiovascular disease prevention in women. Circulation. 2004;109:672–693. - PubMed
-
- Wenger NK. You’ve come a long way, baby: cardiovascular health and disease in women: problems and prospects. Circulation. 2004;109:558–560. - PubMed
-
- Clement DL, De Buyzere ML, De Bacquer DA, de Leeuw PW, Duprez DA, Fagard RH, Gheeraert PJ, Missault LH, Braun JJ, Six RO, Van der Niepen P, O’Brien E, for the Office versus Ambulatory Pressure Study investigators. Prognostic value of ambulatory blood-pressure recordings in patients with treated hypertension. N Engl J Med. 2003;348:2407–2415. - PubMed
-
- Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McClory S, Den Hond E, McCormack P, Staessen JA, O’Brien E. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin Outcome Study. Hypertension. 2005;46:156–161. - PubMed
-
- Hansen TW, Kikuya M, Thijs L, Björklund-Bodegård K, Kuznetsova T, Ohkubo T, Richart T, Torp-Pedersen C, Lind L, Jeppesen J, Ibsen H, Imai Y, Staessen JA, on behalf of the IDACO Investigators. Prognostic superiority of daytime ambulatory over conventional blood pressure in four populations: a meta-analysis of 7030 individuals. J Hypertens. 2007;25:1554–1564. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
