

Development and implementation of a performance improvement project in adult intensive care units: overview of the Improving Medicine Through Pathway Assessment of Critical Therapy in Hospital-Acquired Pneumonia (IMPACT-HAP) study
- PMID: 21266065
- PMCID: PMC3222076
- DOI: 10.1186/cc9988
Development and implementation of a performance improvement project in adult intensive care units: overview of the Improving Medicine Through Pathway Assessment of Critical Therapy in Hospital-Acquired Pneumonia (IMPACT-HAP) study
Abstract
Introduction: In 2005 the American Thoracic Society and Infectious Diseases Society of America (ATS/IDSA) published guidelines for managing hospital-acquired pneumonia (HAP), ventilator-associated pneumonia (VAP), and healthcare-associated pneumonia (HCAP). Although recommendations were evidence based, collective guidelines had not been validated in clinical practice and did not provide specific tools for local implementation. We initiated a performance improvement project designated Improving Medicine Through Pathway Assessment of Critical Therapy in Hospital-Acquired Pneumonia (IMPACT-HAP) at four academic centers in the United States. Our objectives were to develop and implement the project, and to assess compliance with quality indicators in adults admitted to intensive care units (ICUs) with HAP, VAP, or HCAP.
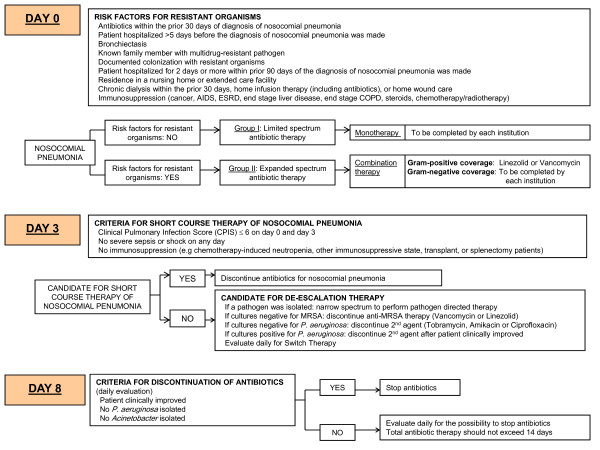
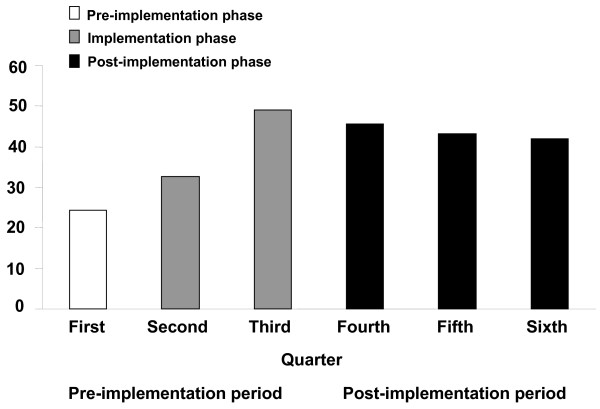
Methods: The project was conducted in three phases over 18 consecutive months beginning 1 February 2006: 1) a three-month planning period for literature review to create the consensus pathway for managing nosocomial pneumonia in these ICUs, a data collection form, quality performance indicators, and internet-based repository; 2) a six-month implementation period for customizing ATS/IDSA guidelines into center-specific guidelines via educational forums; and 3) a nine-month post-implementation period for continuing education and data collection. Data from the first two phases were combined (pre-implementation period) and compared with data from the post-implementation period.
Results: We developed a consensus pathway based on ATS/IDSA guidelines and customized it at the local level to accommodate formulary and microbiologic considerations. We implemented multimodal educational activities to teach ICU staff about the guidelines and continued education throughout post-implementation. We registered 432 patients (pre- vs post-implementation, 274 vs 158). Diagnostic criteria for nosocomial pneumonia were more likely to be met during post-implementation (247/257 (96.1%) vs 150/151 (99.3%); P = 0.06). Similarly, empiric antibiotics were more likely to be compliant with ATS/IDSA guidelines during post-implementation (79/257 (30.7%) vs 66/151 (43.7%); P = 0.01), an effect that was sustained over quarterly intervals (P = 0.0008). Between-period differences in compliance with obtaining cultures and use of de-escalation were not statistically significant.
Conclusions: Developing a multi-center performance improvement project to operationalize ATS/IDSA guidelines for HAP, VAP, and HCAP is feasible with local consensus pathway directives for implementation and with quality indicators for monitoring compliance with guidelines.
Figures
References
-
- Mangino JE, Ford KD, Peyrani P, Kett DH, Zervos MJ, Scerpella E, Ramirez JA. Implementing national guidelines to improve outcomes in patients with hospital-acquired pneumonia: the IMPACT HAP Project. ASHP 42nd Midyear Clinical Meeting; Las Vegas, Nevada. 2007.
-
- Mangino JE, Ramirez JA, Peyrani P, Kett DH, Zervos MJ, Ford KD, Scerpella EG, the IMPACT-HAP Study Group. 18th Annual Scientific Meeting of The Society for Healthcare Epidemiology of America (SHEA) Orlando, Florida; 2008. Development of quality indicators to measure adherence to guidelines in intensive care patients with ventilator-associated, hospital-acquired and healthcare associated pneumonia: the IMPACT-HAP Project (abstract)
-
- Mangino JE, Peyrani P, Kett DH, Zervos MJ, Scerpella EG, Ford KD, Ramirez JA. 48th Annual ICAAC/IDSA 46th Annual Meeting. Washington, DC; 2008. Use of quality indicators to measure compliance with the ATS/IDSA Guidelines for hospital-acquired pneumonia (HAP), healthcare-associated pneumonia (HCAP) and ventilator-associated pneumonia (VAP) at 4 medical centers: the IMPACT-HAP Project (abstract)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
