

Treatment outcome and prognostic factors for patients with bone-only metastases of breast cancer: a single-institution retrospective analysis
- PMID: 21266401
- PMCID: PMC3228079
- DOI: 10.1634/theoncologist.2010-0350
Treatment outcome and prognostic factors for patients with bone-only metastases of breast cancer: a single-institution retrospective analysis
Abstract
Purpose: Limited information is available about the optimal management and clinical outcome of bone-only metastases in breast cancer patients. The objective of this study was to define prognostic factors for patients with bone-only metastases. Our second objective was to compare progression-free survival (PFS) and overall survival (OS) between patients with hormone receptor (HR)(+) tumors and bone-only metastases who received combinatory therapy (chemotherapy followed by endocrine therapy, or endocrine therapy combined with molecular targeted therapy) and those treated with endocrine or chemotherapy alone.
Patients and methods: We retrospectively identified 351 breast cancer patients diagnosed with bone-only metastasis in 1997-2008 at our institution.
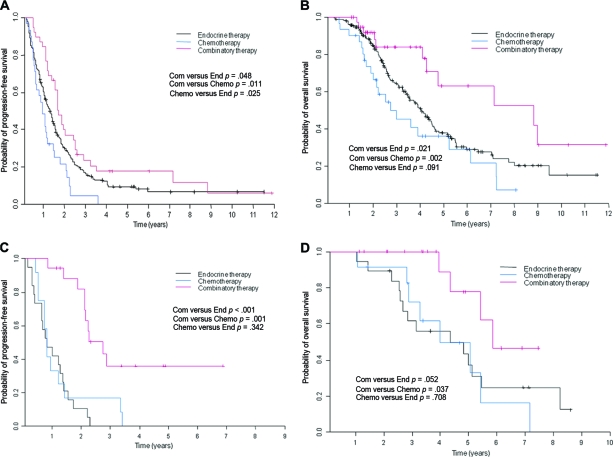
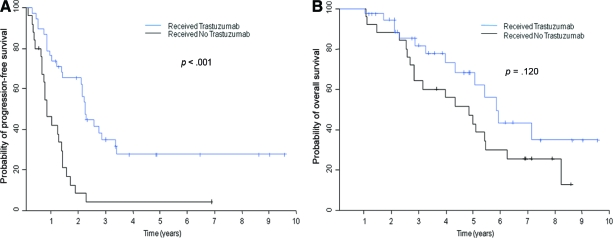
Results: Patients with metastasis detected at the time of their primary breast cancer diagnosis (rather than at recurrence), a single metastasis, or asymptomatic bone disease had a longer PFS interval, and patients with a performance status of 0-1, a single metastasis, or asymptomatic bone disease had a longer OS time. Among patients with HR(+) human epidermal growth factor receptor (HER)-2(-) disease, combinatory therapy was associated with longer PFS and OS times than with endocrine therapy. In multivariate analyses, combinatory therapy was not associated with longer PFS or OS times than with endocrine therapy. Among patients with HER-2(+) disease, trastuzumab led to a longer PFS interval but no difference in the OS time.
Conclusion: Our results indicate that, for HR(+) disease, a prospective trial of chemotherapy followed by endocrine therapy is warranted to determine whether it prolongs survival more than endocrine therapy alone in patients with bone-only metastases.
Conflict of interest statement
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the independent peer reviewers.
Figures
References
-
- Smalley RV, Scogna DM, Malmud LS. Advanced breast cancer with bone-only metastases: A chemotherapeutically responsive pattern of metastases. Am J Clin Oncol. 1982;5:161–166. - PubMed
-
- Swenerton KD, Legha SS, Smith T, et al. Prognostic factors in metastatic breast cancer treated with combination chemotherapy. Cancer Res. 1979;39:1552–1562. - PubMed
-
- Sherry MM, Greco FA, Johnson DH, et al. Metastatic breast cancer confined to the skeletal system. An indolent disease. Am J Med. 1986;81:381–386. - PubMed
-
- Sherry MM, Greco FA, Johnson DH, et al. Breast cancer with skeletal metastases at initial diagnosis. Distinctive clinical characteristics and favorable prognosis. Cancer. 1986;58:178–182. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
