

Effect of pay for performance on the management and outcomes of hypertension in the United Kingdom: interrupted time series study
- PMID: 21266440
- PMCID: PMC3026849
- DOI: 10.1136/bmj.d108
Effect of pay for performance on the management and outcomes of hypertension in the United Kingdom: interrupted time series study
Abstract
Objective: To assess the impact of a pay for performance incentive on quality of care and outcomes among UK patients with hypertension in primary care.
Design: Interrupted time series.
Setting: The Health Improvement Network (THIN) database, United Kingdom.
Participants: 470 725 patients with hypertension diagnosed between January 2000 and August 2007.
Intervention: The UK pay for performance incentive (the Quality and Outcomes Framework), which was implemented in April 2004 and included specific targets for general practitioners to show high quality care for patients with hypertension (and other diseases).
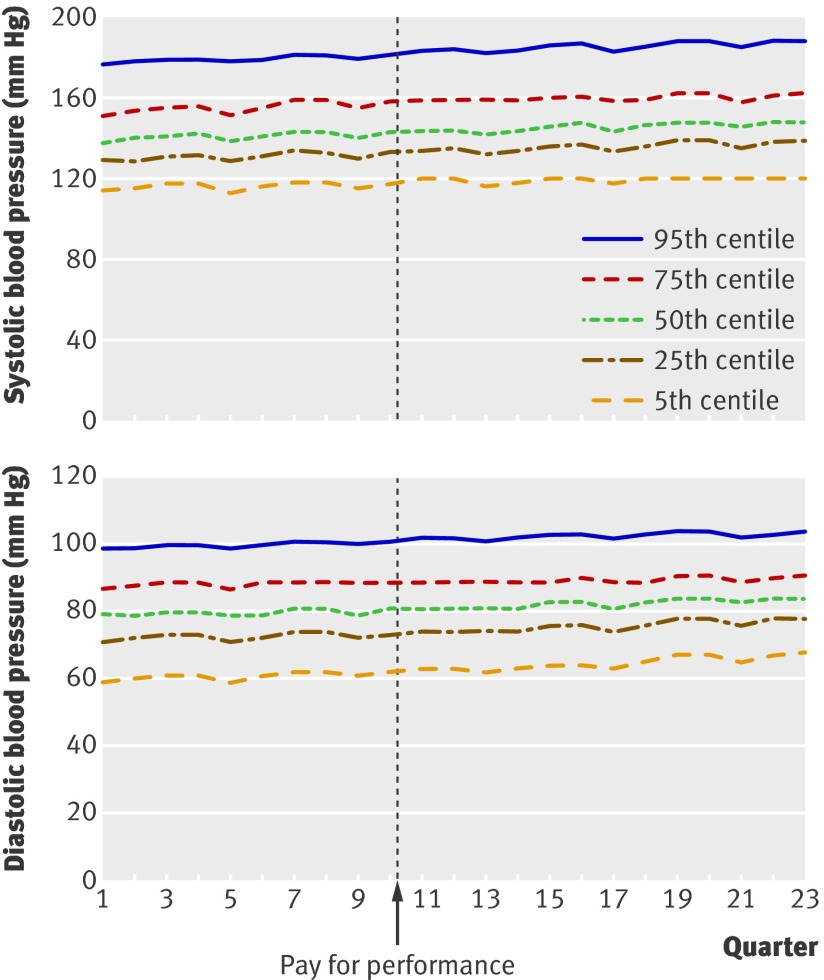
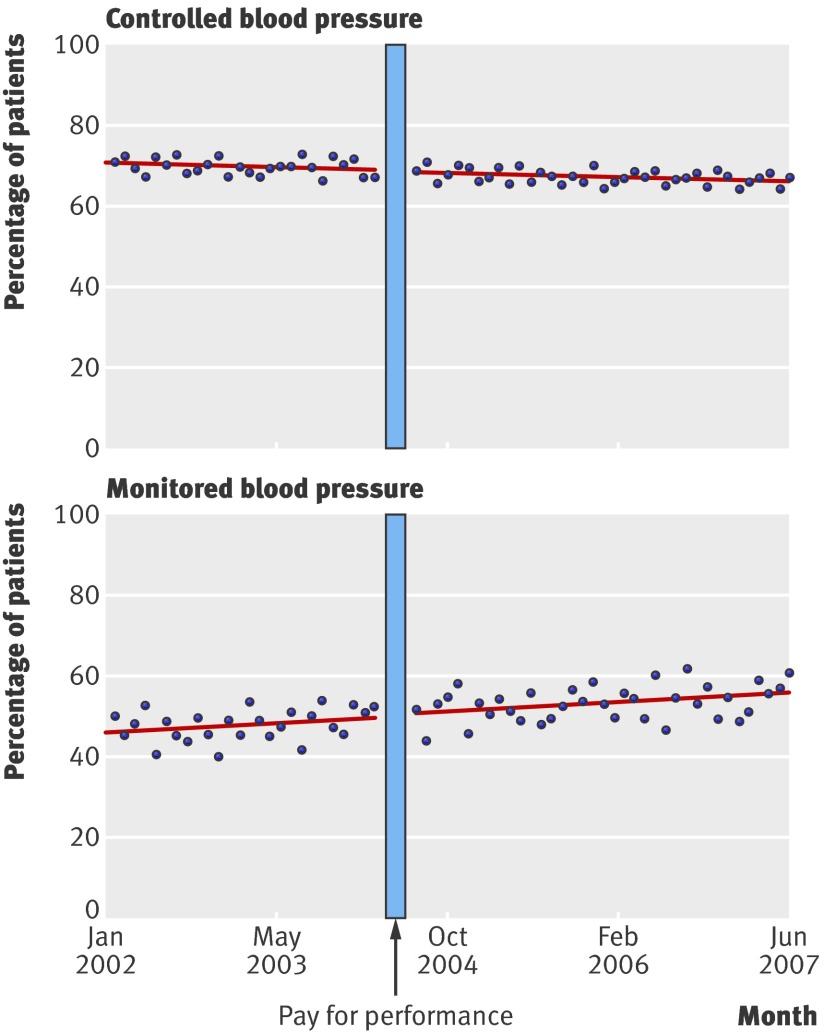
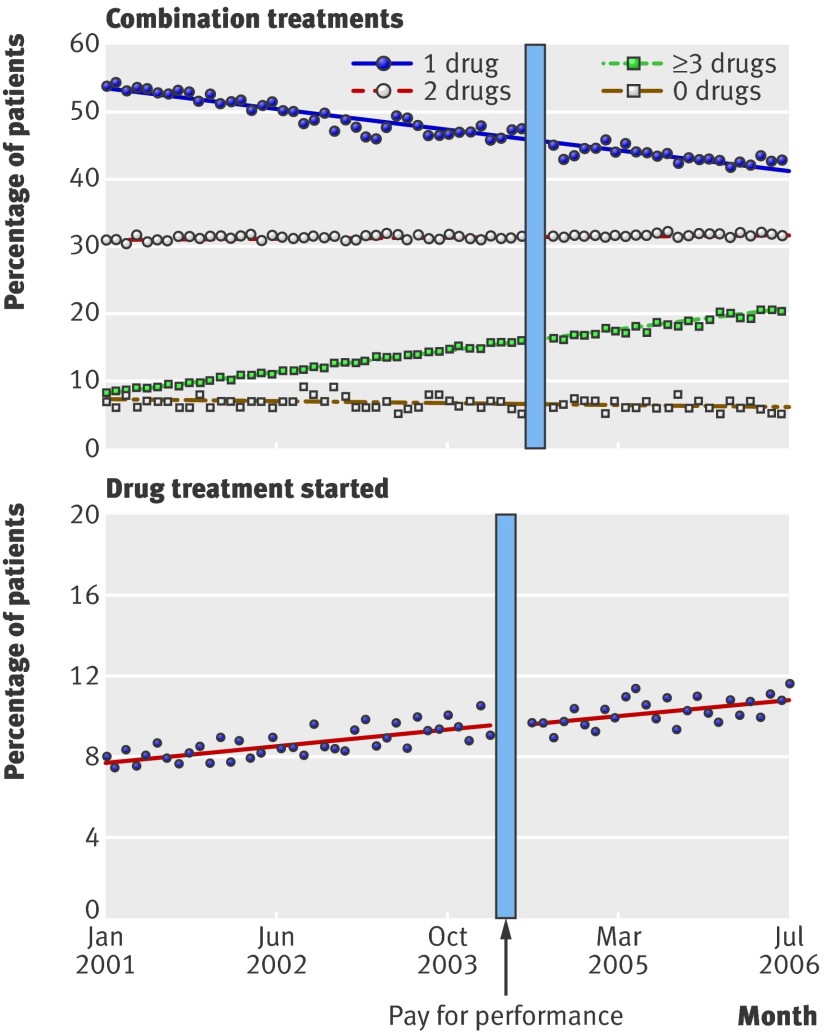
Main outcome measures: Centiles of systolic and diastolic blood pressures over time, rates of blood pressure monitoring, blood pressure control, and treatment intensity at monthly intervals for baseline (48 months) and 36 months after the implementation of pay for performance. Cumulative incidence of major hypertension related outcomes and all cause mortality for subgroups of newly treated (treatment started six months before pay for performance) and treatment experienced (started treatment in year before January 2001) patients to examine different stages of illness.
Results: After accounting for secular trends, no changes in blood pressure monitoring (level change 0.85, 95% confidence interval -3.04 to 4.74, P=0.669 and trend change -0.01, -0.24 to 0.21, P=0.615), control (-1.19, -2.06 to 1.09, P=0.109 and -0.01, -0.06 to 0.03, P=0.569), or treatment intensity (0.67, -1.27 to 2.81, P=0.412 and 0.02, -0.23 to 0.19, P=0.706) were attributable to pay for performance. Pay for performance had no effect on the cumulative incidence of stroke, myocardial infarction, renal failure, heart failure, or all cause mortality in both treatment experienced and newly treated subgroups.
Conclusions: Good quality of care for hypertension was stable or improving before pay for performance was introduced. Pay for performance had no discernible effects on processes of care or on hypertension related clinical outcomes. Generous financial incentives, as designed in the UK pay for performance policy, may not be sufficient to improve quality of care and outcomes for hypertension and other common chronic conditions.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures

Comment in
-
Primary prevention of cardiovascular disease.BMJ. 2011 Jan 25;342:d201. doi: 10.1136/bmj.d201. BMJ. 2011. PMID: 21266415 No abstract available.
-
Effect of pay for performance on hypertension in the United kingdom.Am J Kidney Dis. 2011 Oct;58(4):508-11. doi: 10.1053/j.ajkd.2011.06.010. Epub 2011 Aug 4. Am J Kidney Dis. 2011. PMID: 21816527 No abstract available.
References
-
- Petersen L, Woodard L, Urech T, Daw C, Sookanan S. Does pay for performance improve the quality of health care? Ann Intern Med 2006;145:265-72. - PubMed
-
- Tanenbaum SJ. Pay for performance in Medicare: evidentiary irony and the politics of value. J Health Polit Policy Law 2009;34:717-46. - PubMed
-
- Maynard A, Bloor K. Will financial incentives and penalties improve hospital care? BMJ 2010;340:297-8. - PubMed
-
- Kearney P, Whelton M, Reynolds K, Muntner P, Whelton P, Jiang H. Global burden of hypertension: analysis of worldwide data. Lancet 2005;365:217-23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous