

Living bone allotransplants survive by surgical angiogenesis alone: development of a novel method of composite tissue allotransplantation
- PMID: 21266640
- PMCID: PMC3028450
- DOI: 10.2106/JBJS.G.01152
Living bone allotransplants survive by surgical angiogenesis alone: development of a novel method of composite tissue allotransplantation
Abstract
Background: Segmental bone defects pose reconstructive challenges. Composite tissue allotransplantation offers a potential solution but requires long-term immunosuppression with attendant health risks. This study demonstrates a novel method of composite-tissue allotransplantation, permitting long-term drug-free survival, with use of therapeutic angiogenesis of autogenous vessels to maintain circulation.
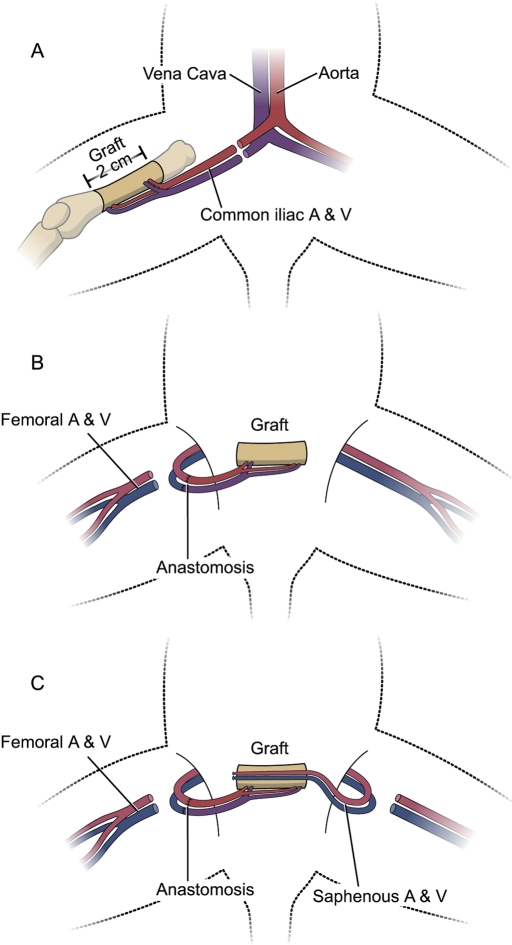
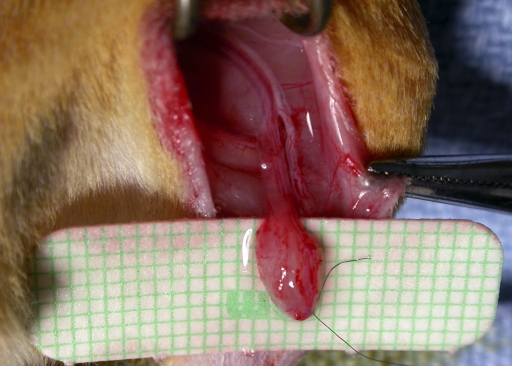
Methods: Ninety-three rats underwent femoral allotransplantation, isotransplantation, or allografting. Group-1 femora were transplanted across a major histocompatibility complex barrier, with microsurgical pedicle anastomoses. The contralateral saphenous artery and vein (termed the AV bundle) of the recipient animal were implanted within the medullary canal to allow development of an autogenous circulation. In Group 2, allotransplantation was also performed, but with AV bundle ligation. Group 3 bones were frozen allografts rather than composite-tissue allotransplantation femora, and Group 4 bones were isotransplants. Paired comparison allowed evaluation of AV bundle effect, bone allogenicity (isogeneic or allogeneic), and initial circulation and viability (allotransplant versus allograft). Two weeks of immunosuppression therapy maintained blood flow initially, during development of a neoangiogenic autogenous blood supply from the AV bundle in patent groups. At eighteen weeks, skin grafts from donor, recipient, and third-party rats were tested for immunocompetence and donor-specific tolerance. At twenty-one weeks, bone circulation was quantified and new bone formation was measured.
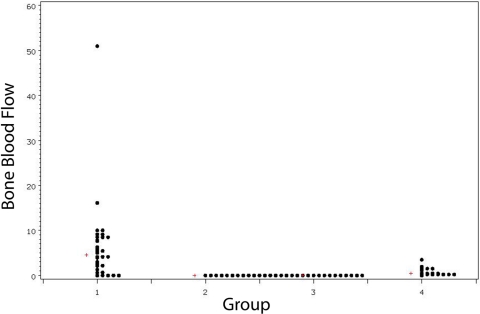
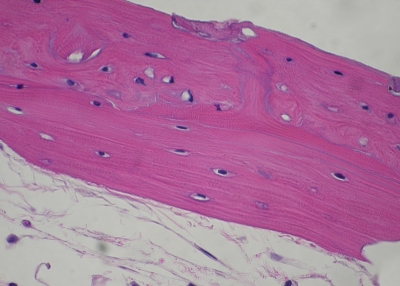
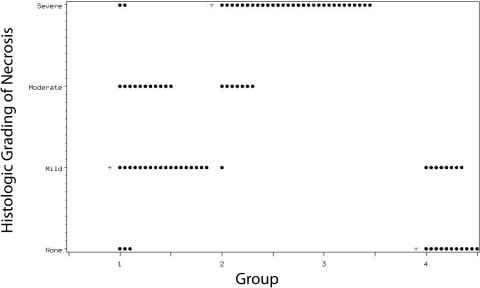
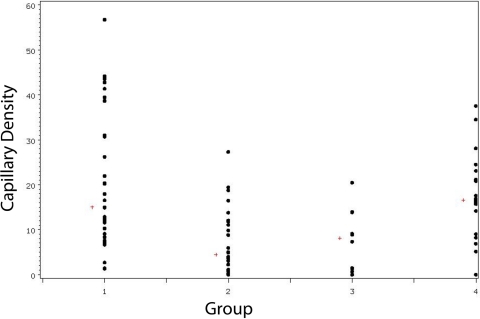
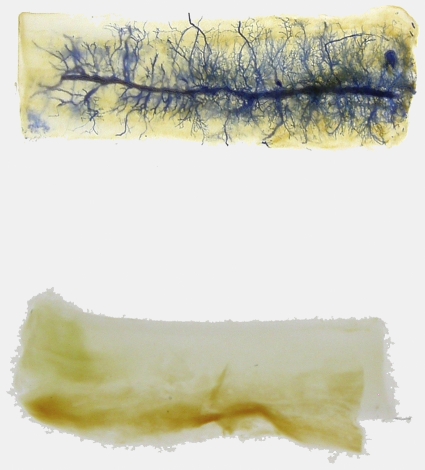
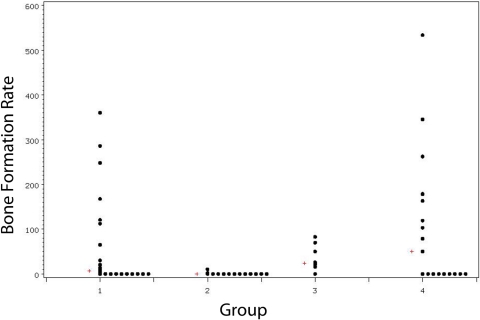
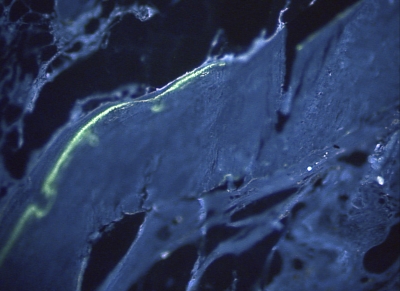
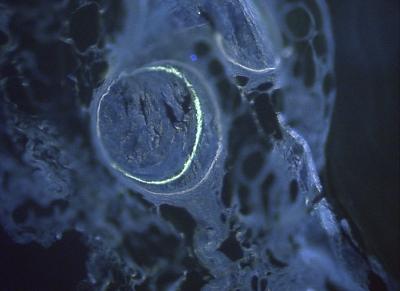
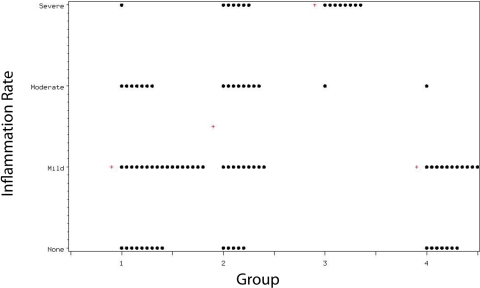
Results: Final circulatory status depended on both the initial viability of the graft and the successful development of neoangiogenic circulation. Median cortical blood flow was highest in Group 1 (4.6 mL/min/100 g), intermediate in Group 4 isotransplants (0.4 mL/min/100 g), and absent in others. Capillary proliferation and new bone formation were generally highest in allotransplants (15.0%, 6.4 μm³/μm²/yr) and isotransplants with patent AV bundles (16.6%, 50.3 μm³/μm²/yr) and less in allotransplants with ligated AV bundles (4.4%, 0.0 μm³/μm²/yr) or allografts (8.1%, 24.1 μm³/μm²/yr). Donor and third-party-type skin grafts were rejected, indicating immunocompetence without donor-specific tolerance.
Conclusions: In the rat model, microvascular allogeneic bone transplantation in combination with short-term immunosuppression and AV bundle implantation creates an autogenous neoangiogenic circulation, permitting long-term allotransplant survival with measurable blood flow.
Figures
References
-
- Bishop AT. Vascularized bone grafting. : Green DP, Hotchkiss RN, Pederson WC, editors Green's operative hand surgery. 4th ed New York: Churchill Livingstone; 1999. p 1221-50
-
- Mankin HJ, Gebhardt MC, Jennings LC, Springfield DS, Tomford WW. Long-term results of allograft replacement in the management of bone tumors. Clin Orthop Relat Res. 1996;324:86-97 - PubMed
-
- Enneking WF, Mindell ER. Observations on massive retrieved human allografts. J Bone Joint Surg Am. 1991;73:1123-42 - PubMed
-
- Heck DA, Chao EY, Sim FH, Pritchard DJ, Shives TC. Titanium fibermetal segmental replacement prostheses. A radiographic analysis and review of current status. Clin Orthop Relat Res. 1986;204:266-85 - PubMed
-
- Abudu A, Carter SR, Grimer RJ. The outcome and functional results of diaphyseal endoprostheses after tumour excision. J Bone Joint Surg Br. 1996;78:652-7 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
