

Correcting mortality for loss to follow-up: a nomogram applied to antiretroviral treatment programmes in sub-Saharan Africa
- PMID: 21267057
- PMCID: PMC3022522
- DOI: 10.1371/journal.pmed.1000390
Correcting mortality for loss to follow-up: a nomogram applied to antiretroviral treatment programmes in sub-Saharan Africa
Abstract
Background: The World Health Organization estimates that in sub-Saharan Africa about 4 million HIV-infected patients had started antiretroviral therapy (ART) by the end of 2008. Loss of patients to follow-up and care is an important problem for treatment programmes in this region. As mortality is high in these patients compared to patients remaining in care, ART programmes with high rates of loss to follow-up may substantially underestimate mortality of all patients starting ART.
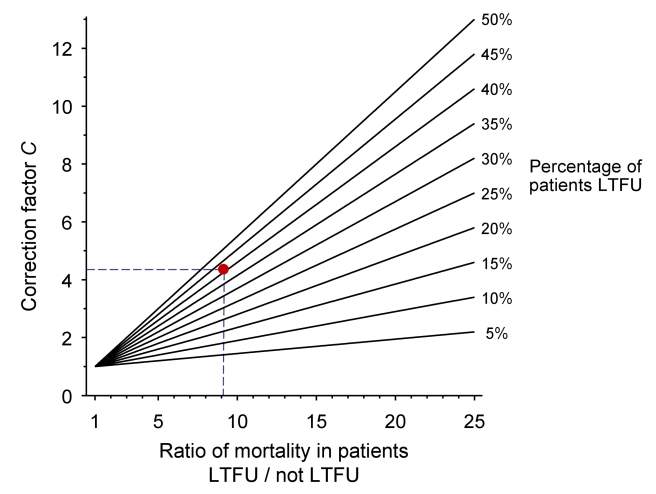
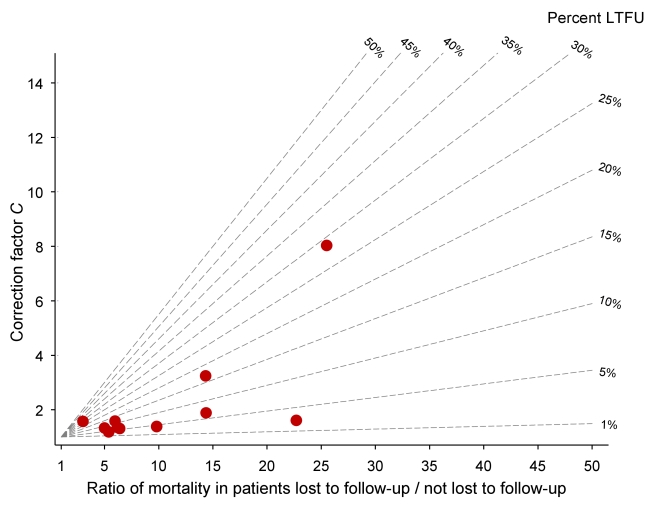
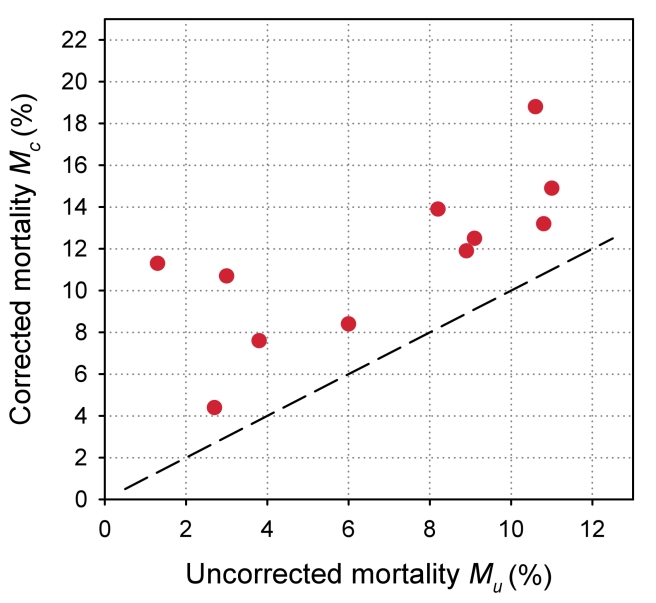
Methods and findings: We developed a nomogram to correct mortality estimates for loss to follow-up, based on the fact that mortality of all patients starting ART in a treatment programme is a weighted average of mortality among patients lost to follow-up and patients remaining in care. The nomogram gives a correction factor based on the percentage of patients lost to follow-up at a given point in time, and the estimated ratio of mortality between patients lost and not lost to follow-up. The mortality observed among patients retained in care is then multiplied by the correction factor to obtain an estimate of programme-level mortality that takes all deaths into account. A web calculator directly calculates the corrected, programme-level mortality with 95% confidence intervals (CIs). We applied the method to 11 ART programmes in sub-Saharan Africa. Patients retained in care had a mortality at 1 year of 1.4% to 12.0%; loss to follow-up ranged from 2.8% to 28.7%; and the correction factor from 1.2 to 8.0. The absolute difference between uncorrected and corrected mortality at 1 year ranged from 1.6% to 9.8%, and was above 5% in four programmes. The largest difference in mortality was in a programme with 28.7% of patients lost to follow-up at 1 year.
Conclusions: The amount of bias in mortality estimates can be large in ART programmes with substantial loss to follow-up. Programmes should routinely report mortality among patients retained in care and the proportion of patients lost. A simple nomogram can then be used to estimate mortality among all patients who started ART, for a range of plausible mortality rates among patients lost to follow-up.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Comment in
-
A simple novel method for determining mortality rates in HIV treatment programs worldwide.PLoS Med. 2011 Jan 18;8(1):e1000392. doi: 10.1371/journal.pmed.1000392. PLoS Med. 2011. PMID: 21267064 Free PMC article.
References
-
- World Health Organization. 2009. Towards universal access. Scaling up priority HIV/AIDS interventions in the health sector. 2009 Progress Report. WHO, Geneva. Available: http://www.who.int/hiv/pub/2009progressreport/en/index.html. Accessed 6 December 2010.
-
- Gilks CF, Crowley S, Ekpini R, Gove S, Perriens J, et al. The WHO public-health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–510. - PubMed
-
- Ivers LC, Kendrick D, Doucette K. Efficacy of antiretroviral therapy programs in resource-poor settings: a meta-analysis of the published literature. Clin Infect Dis. 2005;41:217–224. - PubMed
-
- Keiser O, Orrell C, Egger M, Wood R, Brinkhof MW, et al. Public-health and individual approaches to antiretroviral therapy: township South Africa and Switzerland compared. PLoS Med. 2008;5:e148. doi: 10.1371/journal.pmed.0050148. - DOI - PMC - PubMed
-
- Mills EJ, Nachega JB, Buchan I, Orbinski J, Attaran A, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: A meta-analysis. JAMA. 2006;296:679–690. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
