

Hepatocelluar nodules in liver cirrhosis: hemodynamic evaluation (angiography-assisted CT) with special reference to multi-step hepatocarcinogenesis
- PMID: 21267562
- PMCID: PMC3102849
- DOI: 10.1007/s00261-011-9685-1
Hepatocelluar nodules in liver cirrhosis: hemodynamic evaluation (angiography-assisted CT) with special reference to multi-step hepatocarcinogenesis
Abstract
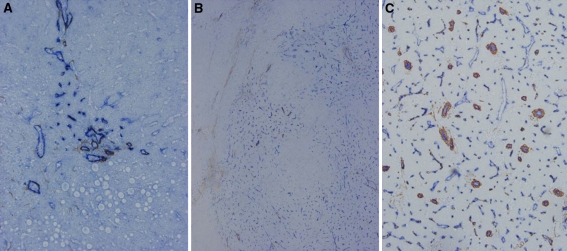
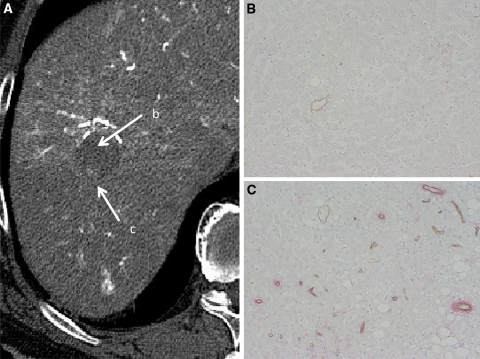
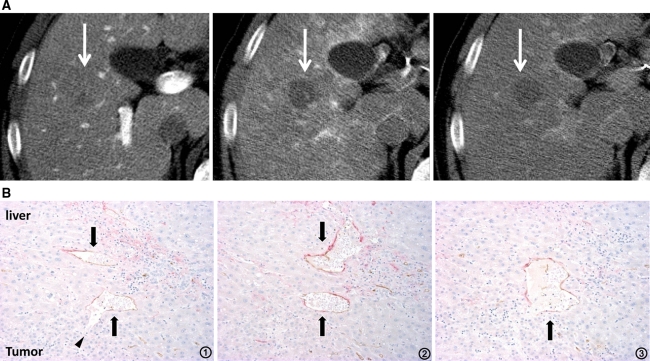
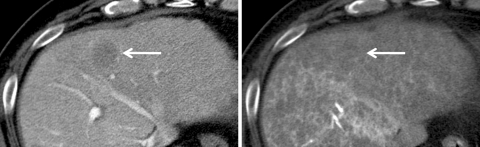
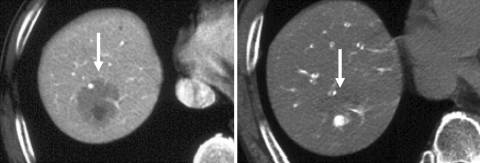
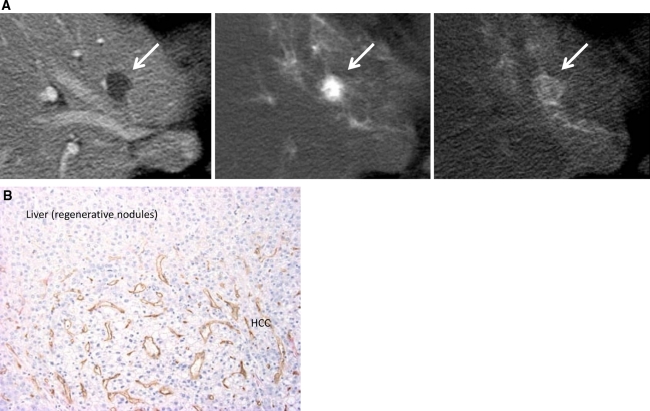
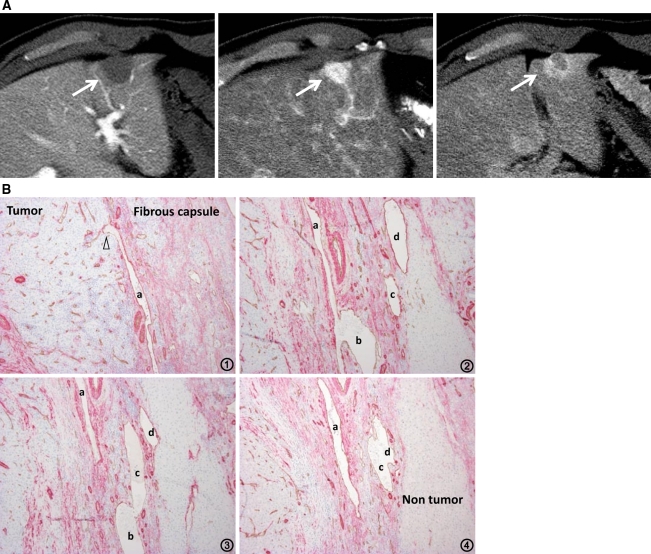
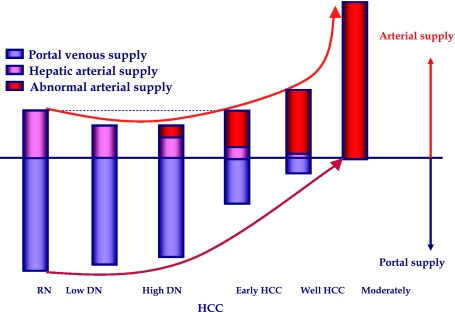
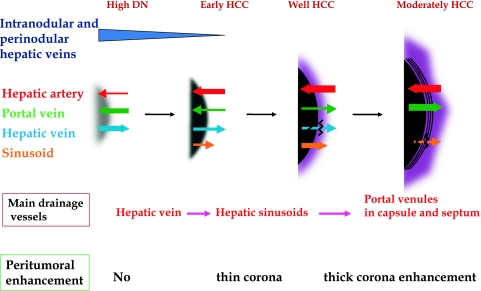
To understand the hemodynamics of hepatocellular carcinoma (HCC) is important for the precise imaging diagnosis and treatment, because there is an intense correlation between their hemodynamics and pathophysiology. Angiogenesis such as sinusoidal capillarization and unpaired arteries shows gradual increase during multi-step hepatocarcinogenesis from high-grade dysplastic nodule to classic hypervascular HCC. In accordance with this angiogenesis, the intranodular portal supply is decreased, whereas the intranodular arterial supply is first decreased during the early stage of hepatocarcinogenesis and then increased in parallel with increasing grade of malignancy of the nodules. On the other hand, the main drainage vessels of hepatocellular nodules change from hepatic veins to hepatic sinusoids and then to portal veins during multi-step hepatocarcinogenesis, mainly due to disappearance of the hepatic veins from the nodules. Therefore, in early HCC, no perinodular corona enhancement is seen on portal to equilibrium phase CT, but it is definite in hypervascular classical HCC. Corona enhancement is thicker in encapsulated HCC and thin in HCC without pseudocapsule. To understand these hemodynamic changes during multi-step hepatocarcinogenesis is important, especially for early diagnosis and treatment of HCCs.
Figures
References
-
- Matsui O, Kadoya M, Suzuki M, et al. Work in progress: dynamic sequential computed tomography during arterial portography in the detection of hepatic neoplasms. Radiology. 1983;146:721–727. - PubMed
-
- Hayashi M, Matsui O, Ueda K, et al. Correlation between the blood supply and grade of malignancy of hepatocellular nodules associated with liver cirrhosis: evaluation by CT during intraarterial injection of contrast medium. AJR Am J Roentgenol. 1999;172:969–976. - PubMed
