

Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold
- PMID: 21269278
- PMCID: PMC3415379
- DOI: 10.1042/CS20100588
Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold
Abstract
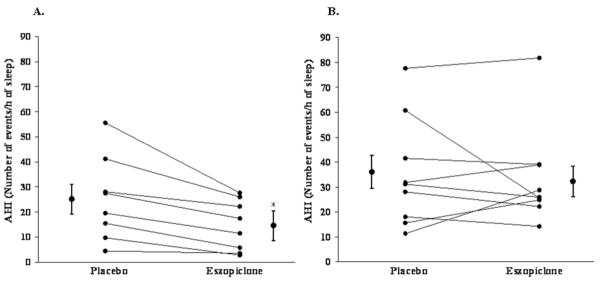
Recent insights into sleep apnoea pathogenesis reveal that a low respiratory arousal threshold (awaken easily) is important for many patients. As most patients experience stable breathing periods mediated by upper-airway dilator muscle activation via accumulation of respiratory stimuli, premature awakening may prevent respiratory stimuli build up as well as the resulting stabilization of sleep and breathing. The aim of the present physiological study was to determine the effects of a non-benzodiazepine sedative, eszopiclone, on the arousal threshold and the AHI (apnoea/hypopnoea index) in obstructive sleep apnoea patients. We hypothesized that eszopiclone would increase the arousal threshold and lower the AHI in patients with a low arousal threshold (0 to -15 cm H(2)O). Following a baseline overnight polysomnogram with an epiglottic pressure catheter to quantify the arousal threshold, 17 obstructive sleep apnoea patients, without major hypoxaemia [nadir SaO(2) (arterial blood oxygen saturation) >70%], returned on two additional nights and received 3 mg of eszopiclone or placebo immediately prior to each study. Compared with placebo, eszopiclone significantly increased the arousal threshold [-14.0 (-19.9 to -10.9) compared with -18.0 (-22.2 to -15.1) cm H(2)O; P<0.01], and sleep duration, improved sleep quality and lowered the AHI without respiratory event prolongation or worsening hypoxaemia. Among the eight patients identified as having a low arousal threshold, reductions in the AHI occurred invariably and were most pronounced (25±6 compared with 14±4 events/h of sleep; P<0.01). In conclusion, eszopiclone increases the arousal threshold and lowers the AHI in obstructive sleep apnoea patients that do not have marked overnight hypoxaemia. The greatest reductions in the AHI occurred in those with a low arousal threshold. The results of this single night physiological study suggest that certain sedatives may be of therapeutic benefit for a definable subgroup of patients. However, additional treatment strategies are probably required to achieve elimination of apnoea.
Figures




References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–1235. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034–2041. - PubMed
-
- Teran-Santos J, Jimenez-Gomez A, Cordero-Guevara J. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. N Engl J Med. 1999;340:847–851. - PubMed
-
- Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, Redline S, Henry JN, Getsy JE, Dinges DF. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis. 1993;147:887–895. - PubMed
-
- Engleman HM, Wild MR. Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS) Sleep Med Rev. 2003;7:81–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials