

Comparing the effect of hydroxyethyl starch 130/0.4 with balanced crystalloid solution on mortality and kidney failure in patients with severe sepsis (6S--Scandinavian Starch for Severe Sepsis/Septic Shock trial): study protocol, design and rationale for a double-blinded, randomised clinical trial
- PMID: 21269526
- PMCID: PMC3040153
- DOI: 10.1186/1745-6215-12-24
Comparing the effect of hydroxyethyl starch 130/0.4 with balanced crystalloid solution on mortality and kidney failure in patients with severe sepsis (6S--Scandinavian Starch for Severe Sepsis/Septic Shock trial): study protocol, design and rationale for a double-blinded, randomised clinical trial
Abstract
Background: By tradition colloid solutions have been used to obtain fast circulatory stabilisation in shock, but high molecular weight hydroxyethyl starch (HES) may cause acute kidney failure in patients with severe sepsis. Now lower molecular weight HES 130/0.4 is the preferred colloid in Scandinavian intensive care units (ICUs) and 1st choice fluid for patients with severe sepsis. However, HES 130/0.4 is largely unstudied in patients with severe sepsis.
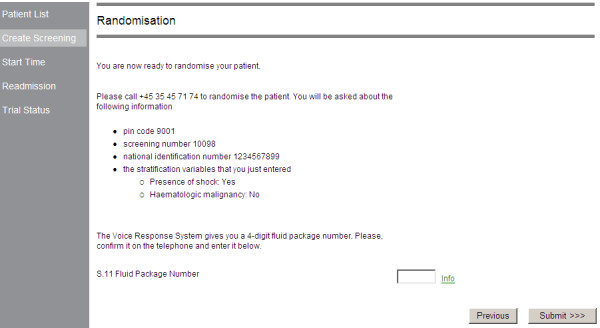
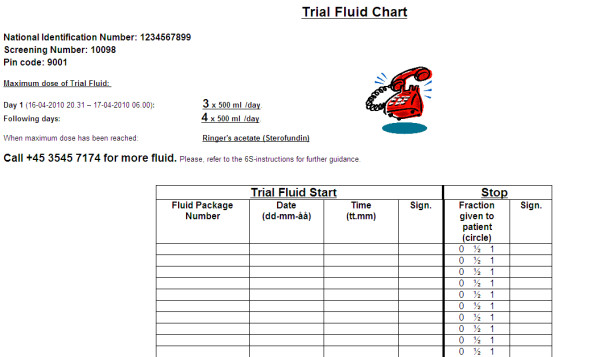
Methods/design: The 6S trial will randomize 800 patients with severe sepsis in 30 Scandinavian ICUs to masked fluid resuscitation using either 6% HES 130/0.4 in Ringer's acetate or Ringer's acetate alone. The composite endpoint of 90-day mortality or end-stage kidney failure is the primary outcome measure. The secondary outcome measures are severe bleeding or allergic reactions, organ failure, acute kidney failure, days alive without renal replacement therapy or ventilator support and 28-day and 1/2- and one-year mortality. The sample size will allow the detection of a 10% absolute difference between the two groups in the composite endpoint with a power of 80%.
Discussion: The 6S trial will provide important safety and efficacy data on the use of HES 130/0.4 in patients with severe sepsis. The effects on mortality, dialysis-dependency, time on ventilator, bleeding and markers of resuscitation, metabolism, kidney failure, and coagulation will be assessed.
Trial registration: ClinicalTrials.gov: NCT00962156.
Figures

References
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med. 2008;34:17–60. doi: 10.1007/s00134-007-0934-2. - DOI - PMC - PubMed
-
- Brunkhorst FM, Engel C, Bloos F, Meier-Hellmann A, Ragaller M, Weiler N, Moerer O, Gruendling M, Oppert M, Grond S, Olthoff D, Jaschinski U, John S, Rossaint R, Welte T, Schaefer M, Kern P, Kuhnt E, Kiehntopf M, Hartog C, Natanson C, Loeffler M, Reinhart K. German Competence Network Sepsis (SepNet) Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008;358:125–139. doi: 10.1056/NEJMoa070716. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
