

Low-dose aspirin therapy in patients with type 2 diabetes and reduced glomerular filtration rate: subanalysis from the JPAD trial
- PMID: 21270185
- PMCID: PMC3024334
- DOI: 10.2337/dc10-1615
Low-dose aspirin therapy in patients with type 2 diabetes and reduced glomerular filtration rate: subanalysis from the JPAD trial
Abstract
Objective: Type 2 diabetes accompanied by renal damage is a strong risk factor for atherosclerotic events. The purpose of this study was to investigate the efficacy of low-dose aspirin therapy on primary prevention of atherosclerotic events in patients with type 2 diabetes and coexisting renal dysfunction.
Research design and methods: The Japanese Primary Prevention of Atherosclerosis With Aspirin for Diabetes (JPAD) trial was a prospective, randomized, open-label trial conducted throughout Japan that enrolled 2,539 type 2 diabetic patients without a history of atherosclerotic diseases. Patients were assigned to the aspirin group (81 mg/day or 100 mg/day) or the nonaspirin group and followed for a median of 4.37 years. The primary end points were atherosclerotic events of fatal and nonfatal ischemic heart disease, stroke, and peripheral arterial disease.
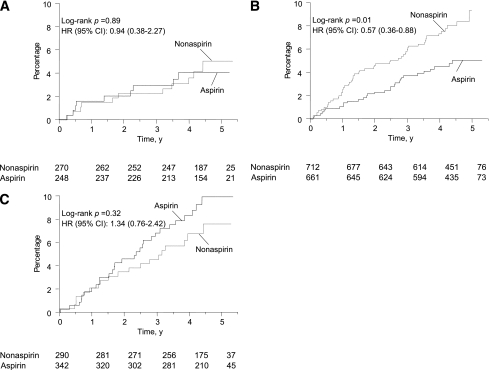
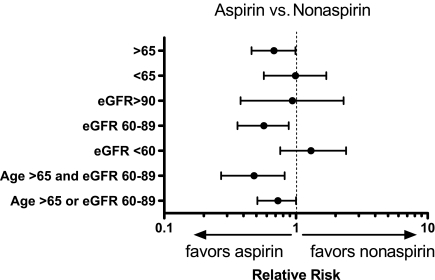
Results: The analysis included 2,523 patients who had serum creatinine measured. In 1,373 patients with baseline estimated glomerular filtration rate (eGFR) 60-89 mL/min/1.73 m(2), the incidence of primary end points was significantly lower in the aspirin group than in the nonaspirin group (aspirin, 30/661; nonaspirin, 55/712; hazard ratio 0.57 [95% CI 0.36-0.88]; P = 0.011). Low-dose aspirin therapy did not reduce primary end points in patients with eGFR ≥ 90 mL/min/1.73 m(2) (aspirin, 9/248; nonaspirin, 11/270; 0.94 [0.38-2.3]) or those with eGFR <60 mL/min/1.73 m(2) (aspirin, 29/342; nonaspirin, 19/290; 1.3 [0.76-2.4]). The Cox proportional hazard model demonstrated a significant interaction between mild renal dysfunction (eGFR 60-89 mL/min/1.73 m(2)) and aspirin (P = 0.02).
Conclusions: These results suggest a differential effect of low-dose aspirin therapy in diabetic patients with eGFR 60-89 mL/min/1.73 m(2).
Trial registration: ClinicalTrials.gov NCT00110448.
Figures
References
-
- Pignone M, Alberts MJ, Colwell JA, et al. American Diabetes Association. American Heart Association. American College of Cardiology Foundation Aspirin for primary prevention of cardiovascular events in people with diabetes: a position statement of the American Diabetes Association, a scientific statement of the American Heart Association, and an expert consensus document of the American College of Cardiology Foundation. Diabetes Care 2010;33:1395–1402 - PMC - PubMed
-
- Mann JF, Gerstein HC, Pogue J, Bosch J, Yusuf S. Renal insufficiency as a predictor of cardiovascular outcomes and the impact of ramipril: the HOPE randomized trial. Ann Intern Med 2001;134:629–636 - PubMed
-
- Anavekar NS, Solomon SD, McMurray JJ, et al. Comparison of renal function and cardiovascular risk following acute myocardial infarction in patients with and without diabetes mellitus. Am J Cardiol 2008;101:925–929 - PubMed
-
- National Kidney Foundation K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39(Suppl. 1):S1–S266 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
