

Best practice wound care
- PMID: 21272244
- PMCID: PMC7950890
- DOI: 10.1111/j.1742-481X.2010.00761.x
Best practice wound care
Abstract
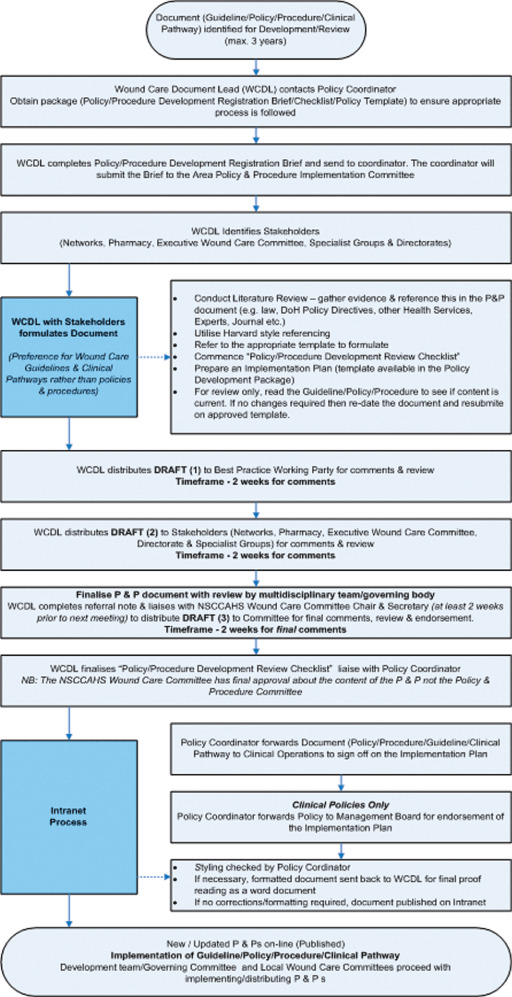
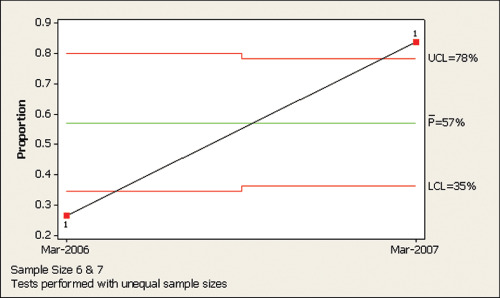
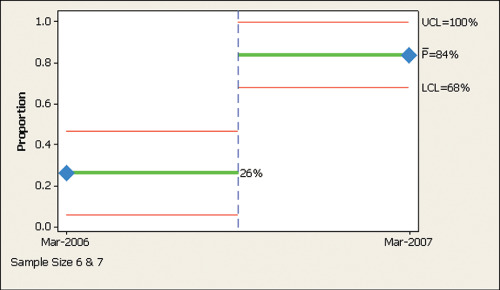
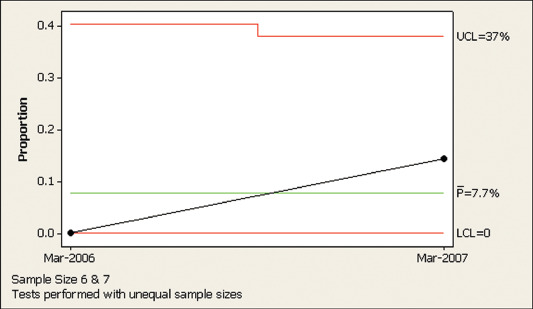
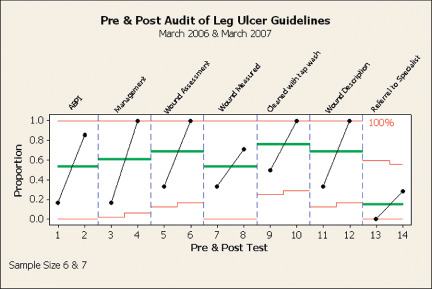
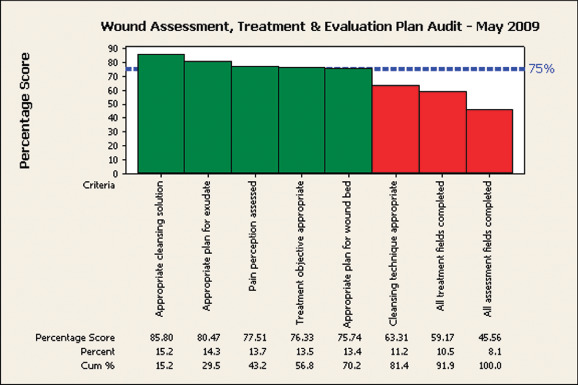
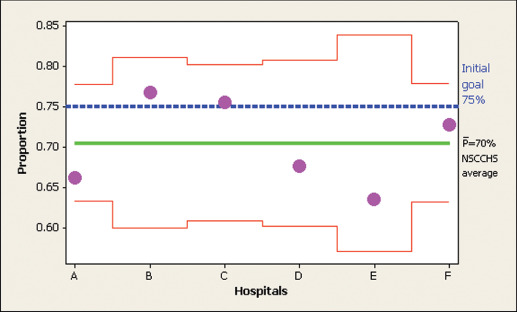
This article describes the barriers, changes and achievements related to implementing one element of a wound care programme being best practice care. With the absence of a coordinated approach to wound care, clinical practice within our Area Health Service (AHS) was diverse, inconsistent and sometimes outdated. This was costly and harmful, leading to overuse of unhelpful care, underuse of effective care and errors in execution. The major aim was to improve the outcomes and quality of life for patients with wound care problems within our community. A collaborative across ten sites/services developed, implemented and evaluated policies and guidelines based on evidence-based bundles of care. Key barriers were local resistance and lack of experience in implementing structural and cultural changes. This was addressed by appointing a wound care programme manager, commissioning of a strategic oversight committee and local wound care committees. The techniques of spread and adoption were used, with early adopters making changes observable and allowing local adaption of guidelines, where appropriate. Deployment and improvement results varied across the sites, ranging from activity but no changes in practice to modest improvement in practice. Evaluating implementation of the leg ulcer guideline as an exemplar, it was demonstrated that there was a statistically significant improvement in overall compliance from 26% to 84%. However, only 7·7% of patients received all interventions to which they were entitled. Compliance with the eight individual interventions of the bundle ranged from 26% to 84%. Generic performance was evaluated against the wound assessment, treatment and evaluation plan with an average compliance of 70%. Early results identified that 20% of wounds were healed within the target of 10 days. As more standardised process are implemented, clinical outcomes should continue to improve and costs decrease.
© 2011 The Authors. © 2011 Blackwell Publishing Ltd and Medicalhelplines.com Inc.
Figures
References
-
- Owen JM. Program evaluation: forms and approaches. Sydney: Allen and Unwin, 1993.
-
- Madsen W, Reid‐Searl K. Overcoming tradition: teaching wound management into the twenty‐first century. Collegian 2007;14:7–10.
-
- Gottrup F. Multidisciplinary wound healing concepts. EWMA J 2003;3:5–11.
-
- NHS Modernisation Agency. Improvement leaders' guide to sustainability and spread. London: Ancient House Printing Group, 2002.
-
- Australian Wound Management Association. Wound awareness campaign 2008 [WWW document]. URL www.elephantintheroom.com.au [accessed on 13 April 2008].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
