

Meta regression analysis to indirectly compare dalteparin to enoxaparin for the prevention of venous thromboembolic events following total hip replacement
- PMID: 21272316
- PMCID: PMC3039553
- DOI: 10.1186/1477-9560-9-3
Meta regression analysis to indirectly compare dalteparin to enoxaparin for the prevention of venous thromboembolic events following total hip replacement
Abstract
Background: Patients undergoing elective total hip replacement (THR) surgery are at an increased risk for venous thromboembolic events (VTEs). Dalteparin and enoxaparin are recommended as thromboprophylaxis for at least 10 days in these patients. Even though both agents have proven clinical effectiveness through placebo controlled studies, there have been no head to head trials to assess comparative effectiveness. Indirect statistical techniques were used to compare safety and efficacy between dalteparin and enoxaparin following THR surgery.
Methods: A literature search was conducted from January 1980 to November 2009 for randomized trials evaluating dalteparin or enoxaparin prophylaxis in THR patients. In trials where a common control was used (e.g. placebo), indirect statistical comparisons between dalteparin and enoxaparin were performed using meta regression analysis with active drug as the primary independent variable.
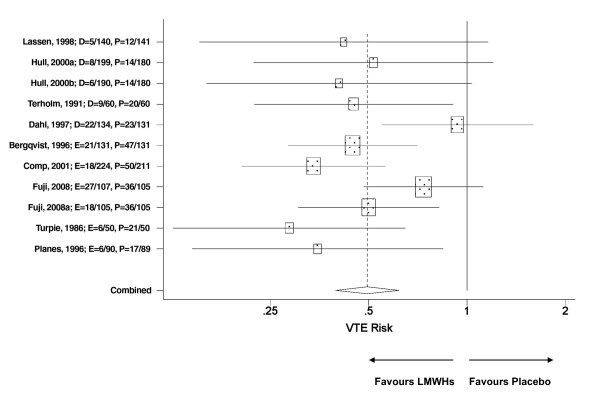
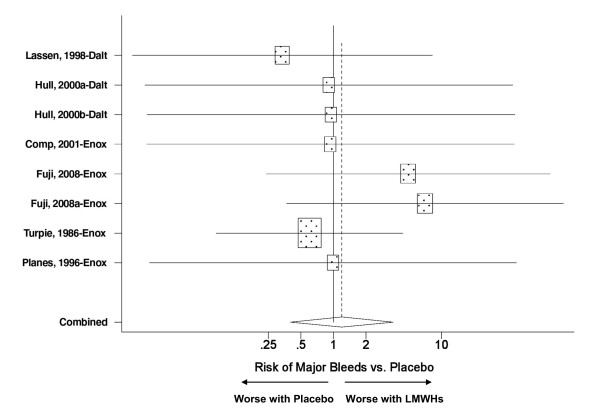
Results: A total of nine placebo controlled enoxaparin (n = 5) and dalteparin (n = 4) trials met the inclusion criteria. THR patients treated with enoxaparin or dalteparin had a 50% VTE risk reduction compared to the placebo control (RR = 0.50, p < 0.001). This benefit was achieved without a significant increase in the risk for major bleeds (RR = 1.19, p = 0.76), heparin induced thrombocytopenia (HIT) (RR = 1.13, p = 0.83) or death (RR = 0.72, p = 0.59). The indirect comparison was not able to find significant differences between enoxaparin and dalteparin in terms of VTEs (p = 0.36), major bleeds (p = 0.45), HIT (p = 0.48) and death (p = 0.86).
Conclusions: The findings suggested comparable safety and efficacy between dalteparin and enoxaparin in TKR patients. Therefore, treatment decisions should be based on other considerations, such as patient or physician preference, ease of administration and cost.
Figures
Similar articles
-
Meta-regression analysis to indirectly compare prophylaxis with dalteparin or enoxaparin in patients at high risk for venous thromboembolic events.Clin Appl Thromb Hemost. 2012 Jun;18(3):233-42. doi: 10.1177/1076029611426869. Epub 2012 Mar 2. Clin Appl Thromb Hemost. 2012. PMID: 22387576 Review.
-
Extended dalteparin prophylaxis for venous thromboembolic events: cost-utility analysis in patients undergoing major orthopedic surgery.Am J Cardiovasc Drugs. 2009;9(1):45-58. doi: 10.2165/00129784-200909010-00005. Am J Cardiovasc Drugs. 2009. PMID: 19178131
-
Budget Impact of Rivaroxaban for the Prevention of Thromboembolic Events after Hip or Knee Replacement in Spain.J Health Econ Outcomes Res. 2016 Jan 28;4(1):35-46. doi: 10.36469/9824. eCollection 2016. J Health Econ Outcomes Res. 2016. PMID: 34430666 Free PMC article.
-
Pharmacoeconomic evaluation of dabigatran, rivaroxaban and apixaban versus enoxaparin for the prevention of venous thromboembolism after total hip or knee replacement in Spain.Pharmacoeconomics. 2014 Sep;32(9):919-36. doi: 10.1007/s40273-014-0175-5. Pharmacoeconomics. 2014. PMID: 24895235
-
Dabigatran etexilate for the prevention of venous thromboembolism in patients undergoing elective hip or knee surgery: a NICE single technology appraisal.Pharmacoeconomics. 2012 Feb 1;30(2):137-46. doi: 10.2165/11591590-000000000-00000. Pharmacoeconomics. 2012. PMID: 22185183 Review.
Cited by
-
Venous Thromboembolism (VTE) Prophylaxis for Hip and Knee Arthroplasty: Changing Trends.Curr Rev Musculoskelet Med. 2014 Jun;7(2):108-16. doi: 10.1007/s12178-014-9207-1. Curr Rev Musculoskelet Med. 2014. PMID: 24706152 Free PMC article.
-
A cost-utility analysis of dabigatran, enoxaparin, and usual care for venous thromboprophylaxis after hip or knee replacement surgery in Thailand.J Thromb Thrombolysis. 2017 Feb;43(2):252-262. doi: 10.1007/s11239-016-1433-5. J Thromb Thrombolysis. 2017. PMID: 27704332
References
-
- Landefeld CS, Ilanus P. Prevention of Venous Thrombosis. New York, NY: Marcel Dekker; 1993. Economic burden of venous thromboembolism; pp. 69–85.
LinkOut - more resources
Full Text Sources
Miscellaneous
