

Multidisciplinary team care may slow the rate of decline in renal function
- PMID: 21273376
- PMCID: PMC3069359
- DOI: 10.2215/CJN.06610810
Multidisciplinary team care may slow the rate of decline in renal function
Abstract
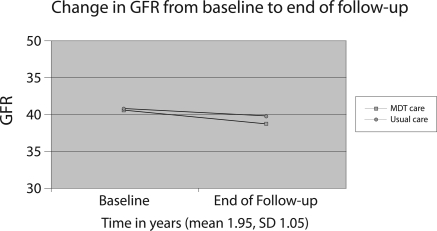
Background and objectives: A multidisciplinary team (MDT) approach to chronic kidney disease (CKD) may help optimize care of CKD and comorbidities. We implemented an MDT quality improvement project for persons with stage 3 CKD and comorbid diabetes and/or hypertension. Our objective was to decrease the rate of decline of GFR.
Design, setting, participants, & measurements: We used a 4-year historical cohort to compare 1769 persons referred for usual nephrology care versus 233 referred for MDT care within an integrated, not-for-profit Health Maintenance Organization (HMO). Usual care consisted of referral to an outside nephrologist. The MDT consisted of an HMO-based nephrologist, pharmacy specialist, diabetes educator, dietitian, social worker, and nephrology nurse. Both groups received usual primary care. The primary outcome was rate of decline of GFR. Secondary outcomes were LDL, hemoglobin A1c, and BP.
Results: In multivariate repeated-measures analyses, MDT care was associated with a mean annual decline in GFR of 1.2 versus 2.5 ml/min per 1.73 m(2) for usual care. In stratified analyses, the significant difference in GFR decline persisted only in those who completed their referrals. There were no differences in the secondary outcomes between groups.
Conclusions: In this integrated care setting, MDT care resulted in a slower decline in GFR than usual care. This occurred despite a lack of significant differences for secondary disease-specific measures, suggesting that other differences in the MDT population or care process accounted for the slower decline in GFR in the MDT group.
© 2011 by the American Society of Nephrology
Figures
References
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van LF, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- United States Renal Data System: USRDS 2010 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2010, Tables CII and DII
-
- Whaley-Connell AT, Sowers JR, Stevens LA, McFarlane SI, Shlipak MG, Norris KC, Chen SC, Qiu Y, Wang C, Li S, Vassalotti JA, Collins AJ: CKD in the United States: Kidney Early Evaluation Program (KEEP) and National Health and Nutrition Examination Survey (NHANES) 1999–2004. Am J Kidney Dis 51: S13–S20, 2008 - PubMed
-
- Gullion CM, Keith DS, Nichols GA, Smith DH: Impact of comorbidities on mortality in managed care patients with CKD. Am J Kidney Dis 48: 212–220, 2006 - PubMed
-
- Nissenson AR, Collins AJ, Hurley J, Petersen H, Pereira BJ, Steinberg EP: Opportunities for improving the care of patients with chronic renal insufficiency: Current practice patterns. J Am Soc Nephrol 12: 1713–1720, 2001 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
