

The possible protective role of glucagon-like peptide 1 on endothelium during the meal and evidence for an "endothelial resistance" to glucagon-like peptide 1 in diabetes
- PMID: 21273492
- PMCID: PMC3041210
- DOI: 10.2337/dc10-1949
The possible protective role of glucagon-like peptide 1 on endothelium during the meal and evidence for an "endothelial resistance" to glucagon-like peptide 1 in diabetes
Abstract
Objective: Glucagon-like peptide 1 (GLP-1) stimulates insulin secretion. However, GLP-1 also improves endothelial function in diabetes.
Research design and methods: Sixteen type 2 diabetic patients and 12 control subjects received a meal, an oral glucose tolerance test (OGTT), and two hyperglycemic clamps, with or without GLP-1. The clamps were repeated in diabetic patients after 2 months of strict glycemic control.
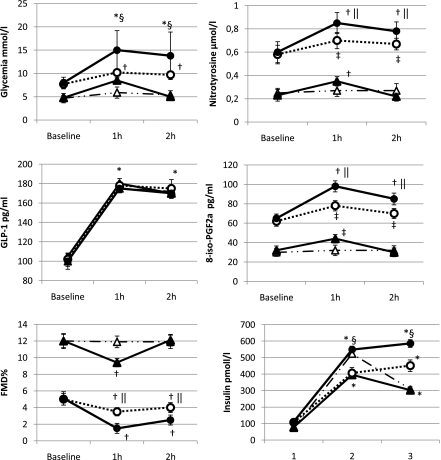
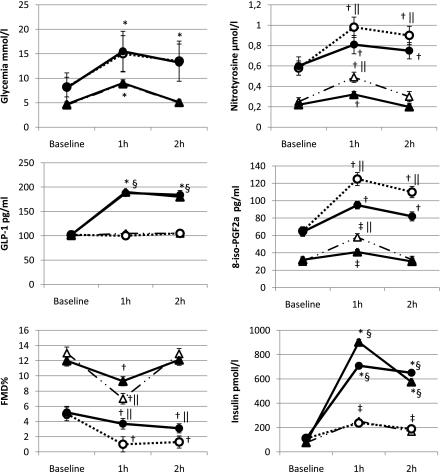
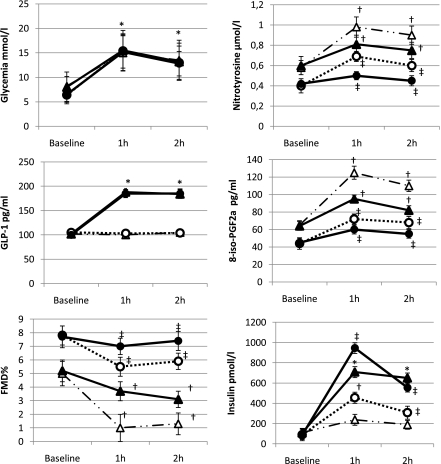
Results: During the meal, glycemia, nitrotyrosine, and plasma 8-iso prostaglandin F2α (8-iso-PGF2a) remained unchanged in the control subjects, whereas they increased in diabetic patients. Flow-mediated vasodilation (FMD) decreased in diabetes, whereas GLP-1 increased in both groups. During the OGTT, an increase in glycemia, nitrotyrosine, and 8-iso-PGF2a and a decrease in FMD were observed at 1 h in the control subjects and at 1 and 2 h in the diabetic patients. In the same way, GLP-1 increased in both groups at the same levels of the meal. During the clamps, in both the control subjects and the diabetic patients, a significant increase in nitrotyrosine and 8-iso-PGF2a and a decrease in FMD were observed, effects that were significantly reduced by GLP-1. After improved glycemic control, hyperglycemia during the clamps was less effective in producing oxidative stress and endothelial dysfunction and the GLP-1 administration was most effective in reducing these effects.
Conclusions: Our data suggest that during the meal GLP-1 can simultaneously exert an incretin effect on insulin secretion and a protective effect on endothelial function, reasonably controlling oxidative stress generation. The ability of GLP-1 in protecting endothelial function seems to depend on the level of glycemia, a phenomenon already described for insulin secretion.
Figures
References
-
- Drucker DJ. Minireview: the glucagon-like peptides. Endocrinology 2001;142:521–527 - PubMed
-
- Ceriello A. Postprandial hyperglycemia and diabetes complications: is it time to treat? Diabetes 2005;54:1–7 - PubMed
-
- Ross R. The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 1993;362:801–809 - PubMed
-
- Peters A. Incretin-based therapies: review of current clinical trial data. Am J Med 2010;123(Suppl.):S28–S37 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
