

The cost-effectiveness of personalized genetic medicine: the case of genetic testing in neonatal diabetes
- PMID: 21273495
- PMCID: PMC3041194
- DOI: 10.2337/dc10-1616
The cost-effectiveness of personalized genetic medicine: the case of genetic testing in neonatal diabetes
Abstract
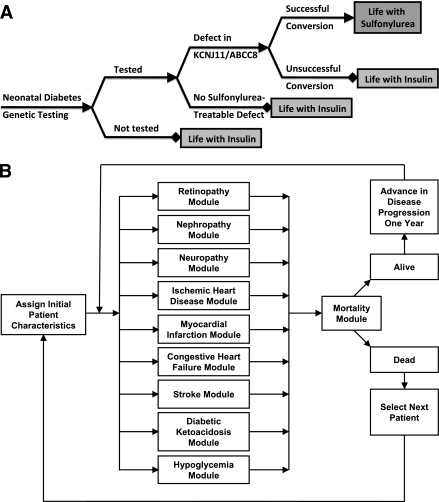
Objective: Neonatal diabetes mellitus is a rare form of diabetes diagnosed in infancy. Nearly half of patients with permanent neonatal diabetes have mutations in the genes for the ATP-sensitive potassium channel (KCNJ11 and ABCC8) that allow switching from insulin to sulfonylurea therapy. Although treatment conversion has dramatic benefits, the cost-effectiveness of routine genetic testing is unknown.
Research design and methods: We conducted a societal cost-utility analysis comparing a policy of routine genetic testing to no testing among children with permanent neonatal diabetes. We used a simulation model of type 1 diabetic complications, with the outcome of interest being the incremental cost-effectiveness ratio (ICER, $/quality-adjusted life-year [QALY] gained) over 30 years of follow-up.
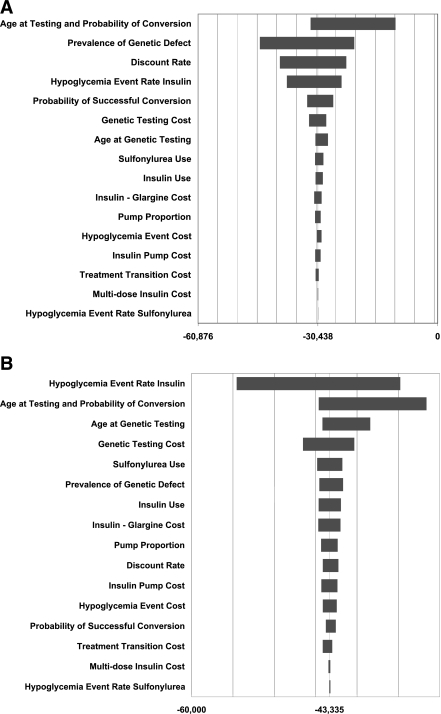
Results: In the base case, the testing policy dominated the no-testing policy. The testing policy was projected to bring about quality-of-life benefits that enlarged over time (0.32 QALYs at 10 years, 0.70 at 30 years) and produced savings in total costs that were present as early as 10 years ($12,528 at 10 years, $30,437 at 30 years). Sensitivity analyses indicated that the testing policy would remain cost-saving as long as the prevalence of the genetic defects remained >3% and would retain an ICER <$200,000/QALY at prevalences between 0.7 and 3%.
Conclusions: Genetic testing in neonatal diabetes improves quality of life and lowers costs. This paradigmatic case study highlights the potential economic impact of applying the concepts of personalized genetic medicine to other disorders in the future.
Figures
References
-
- Grulich-Henn J, Wagner V, Thon A, et al. Entities and frequency of neonatal diabetes: data from the diabetes documentation and quality management system (DPV). Diabet Med 2010;27:709–712 - PubMed
-
- Gloyn AL, Pearson ER, Antcliff JF, et al. Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med 2004;350:1838–1849 - PubMed
-
- Babenko AP, Polak M, Cavé H, et al. Activating mutations in the ABCC8 gene in neonatal diabetes mellitus. N Engl J Med 2006;355:456–466 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
